

Higher New York Heart Association classes and increased mortality and hospitalization in patients with heart failure and preserved left ventricular function
- PMID: 16442912
- PMCID: PMC2771182
- DOI: 10.1016/j.ahj.2005.03.066
Higher New York Heart Association classes and increased mortality and hospitalization in patients with heart failure and preserved left ventricular function
Abstract
Background: The association between higher New York Heart Association (NYHA) class and outcomes in patients with heart failure and preserved systolic function is not well known.
Methods: We performed a retrospective follow-up study of 988 patients with heart failure with ejection fraction > 45% who participated in the DIG trial. Using Cox proportional hazard models, we estimated risks and all-cause mortality, heart failure mortality, all-cause hospitalization, and hospitalization due to worsening heart failure during a median follow-up of 38.5 months.
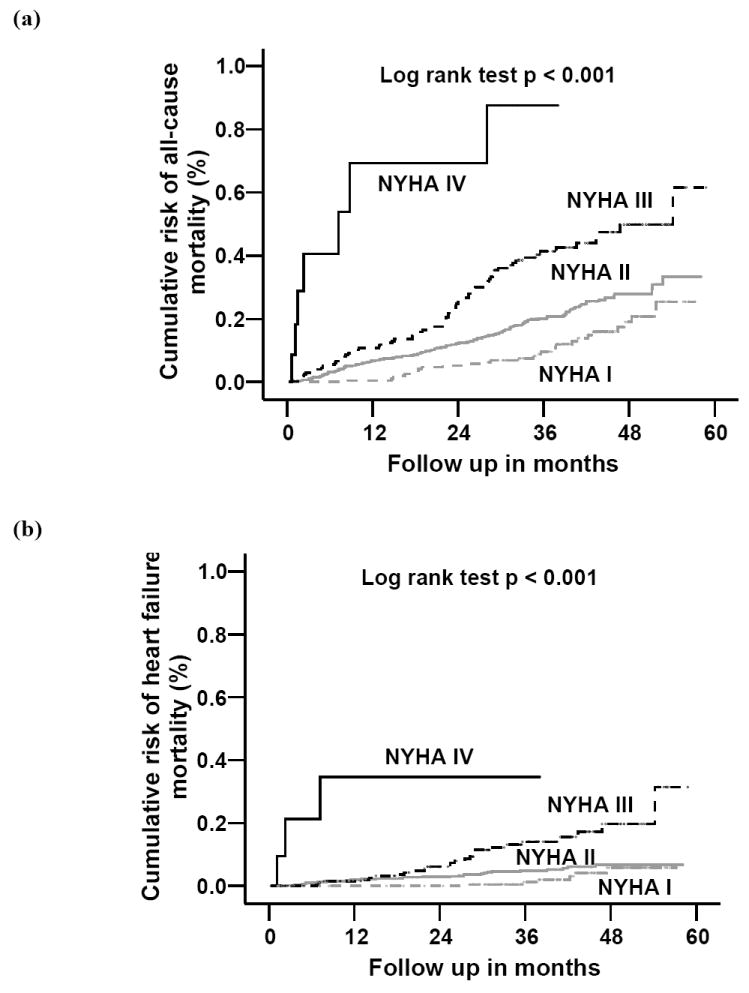
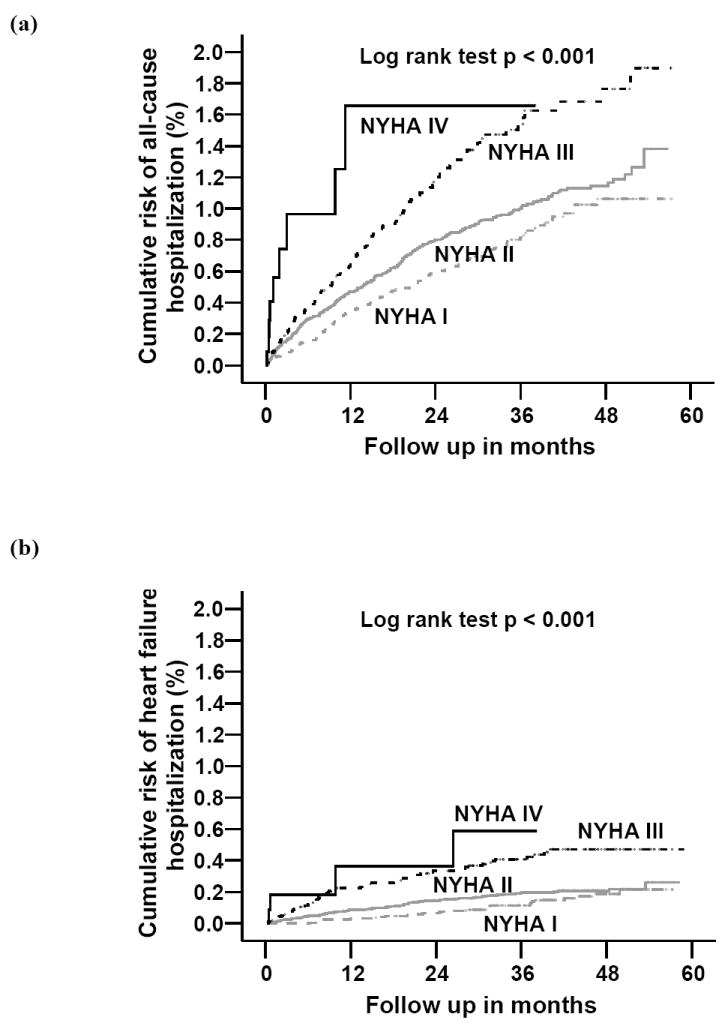
Results: Patients had a median age of 68 years; 41.2% were women and 13.9%, nonwhites. Overall, 23.4% of patients died, and 19.9% were hospitalized because of worsening heart failure. Proportion of patients with NYHA classes I, II, III, and IV were 19.9%, 58.0%, 20.9%, and 1.2%, respectively, and 14.7%, 21.1%, 35.9%, and 58.3%, respectively, died of all causes (P < .001 for trend). Respective rates for heart failure-related hospitalizations were 14.2%, 17.1%, 32.5%, and 33.3% (P < .001 for trend). Compared with NYHA class I patients, adjusted hazard ratios (HRs) for all-cause mortality for class II, III, and IV patients were 1.54 (95% CI 1.02-2.32, P = .042), 2.56 (95% CI 1.64-24.01, P < .001), and 8.46 (95% CI 3.57-20.03, P < .001), respectively. Respective adjusted HRs (95% CI) for hospitalization due to heart failure for class II, III, and IV patients were 1.16 (0.76-1.77) (P = .502), 2.27 (1.45-3.56) (P < .001), and 3.71 (1.25-11.02) (P = 018). New York Heart Association classes II through IV were also associated with higher risk of all-cause hospitalization.
Conclusion: Higher NYHA classes were associated with poorer outcomes in patients with heart failure and preserved systolic function.
Figures
References
-
- Scrutinio D, Lagioia R, Ricci A, Clemente M, Boni L, Rizzon P. Prediction of mortality in mild to moderately symptomatic patients with left ventricular dysfunction. The role of the New York Heart Association classification, cardiopulmonary exercise testing, two-dimensional echocardiography and Holter monitoring. Eur Heart J. 1994;15:1089–95. - PubMed
-
- Madsen BK, Hansen JF, Stokholm KH, Brons J, Husum D, Mortensen LS. Chronic congestive heart failure. Description and survival of 190 consecutive patients with a diagnosis of chronic congestive heart failure based on clinical signs and symptoms. Eur Heart J. 1994;15:303–10. - PubMed
-
- Muntwyler J, Abetel G, Gruner C, Follath F. One-year mortality among unselected outpatients with heart failure. Eur Heart J. 2002;23:1861–6. - PubMed
-
- Horwich TB, Fonarow GC, Hamilton MA, MacLellan WR, Borenstein J. Anemia is associated with worse symptoms, greater impairment in functional capacity and a significant increase in mortality in patients with advanced heart failure. J Am Coll Cardiol. 2002;39:1780–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
