

Using a combination of click- and tone burst-evoked auditory brain stem response measurements to estimate pure-tone thresholds
- PMID: 16446565
- PMCID: PMC2441480
- DOI: 10.1097/01.aud.0000194511.14740.9c
Using a combination of click- and tone burst-evoked auditory brain stem response measurements to estimate pure-tone thresholds
Abstract
Design: A retrospective medical record review of evoked potential and audiometric data were used to determine the accuracy with which click-evoked and tone burst-evoked auditory brain stem response (ABR) thresholds predict pure-tone audiometric thresholds.
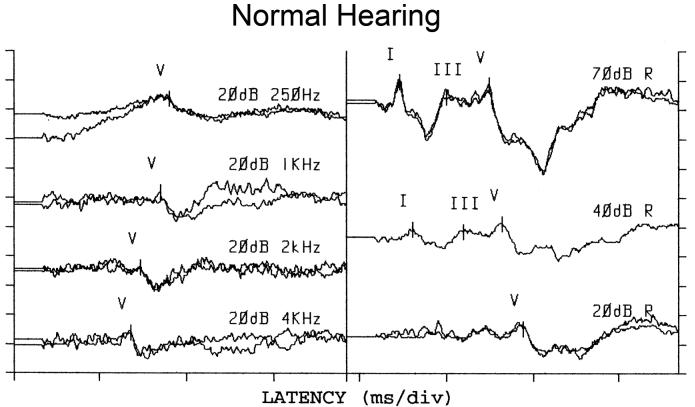
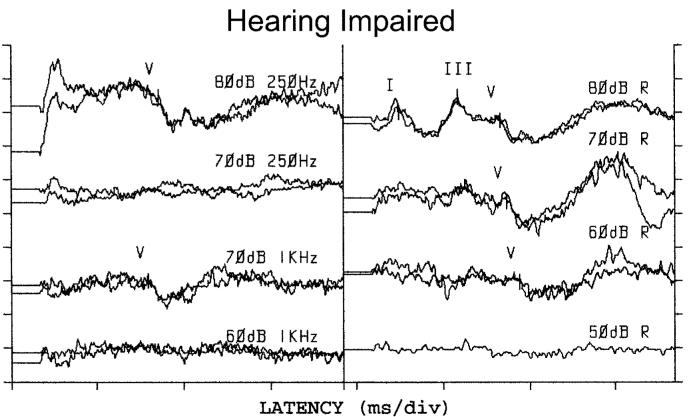
Methods: The medical records were reviewed of a consecutive group of patients who were referred for ABR testing for audiometric purposes over the past 4 yrs. ABR thresholds were measured for clicks and for several tone bursts, including a single-cycle, Blackman-windowed, 250-Hz tone burst, which has a broad spectrum with little energy above 600 Hz. Typically, the ABR data were collected because the patients were unable to provide reliable estimates of hearing sensitivity, based on behavioral test techniques, due to developmental level. Data were included only if subsequently obtained behavioral audiometric data were available to which the ABR data could be compared. Almost invariably, the behavioral data were collected after the ABR results were obtained. Because of this, data were included on only those ears for which middle ear tests (tympanometry, otoscopic examination, pure-tone air- and bone-conduction thresholds) indicated that middle ear status was similar at the times of both tests. With these inclusion criteria, data were available on 140 ears of 77 subjects.
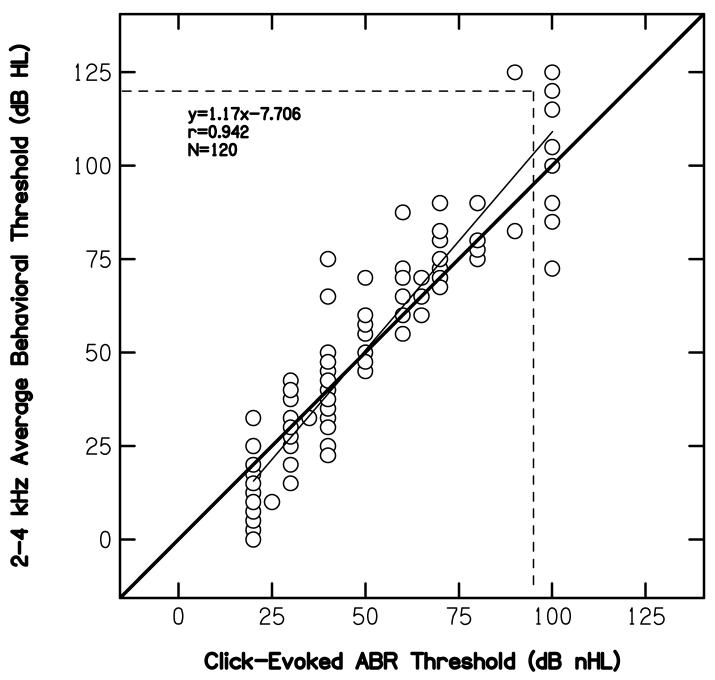
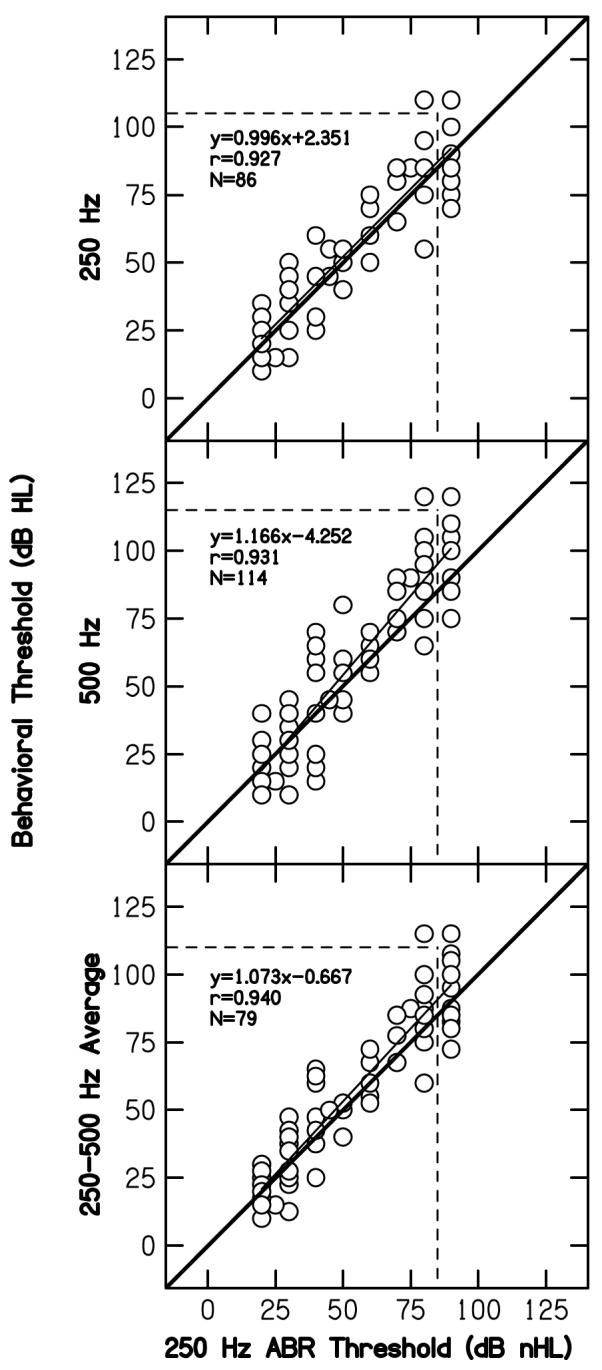
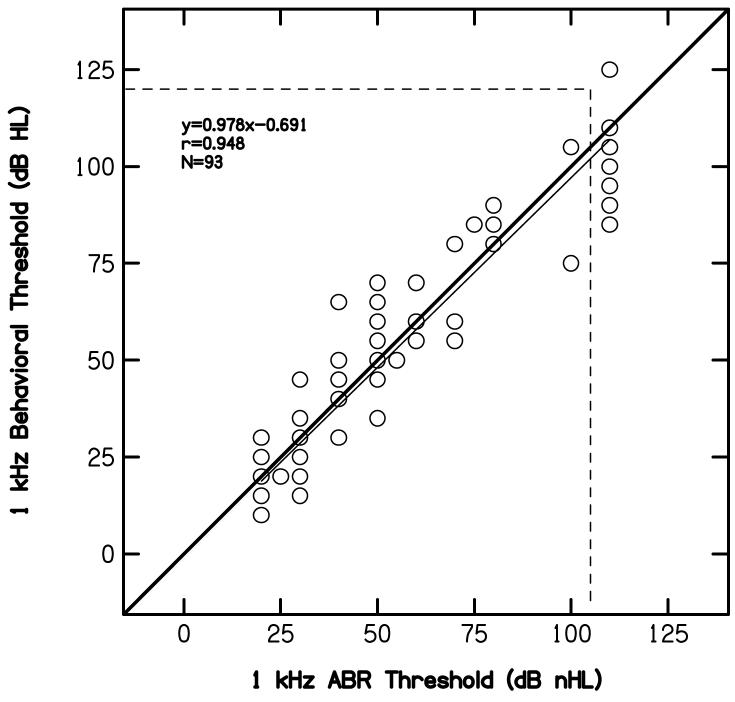
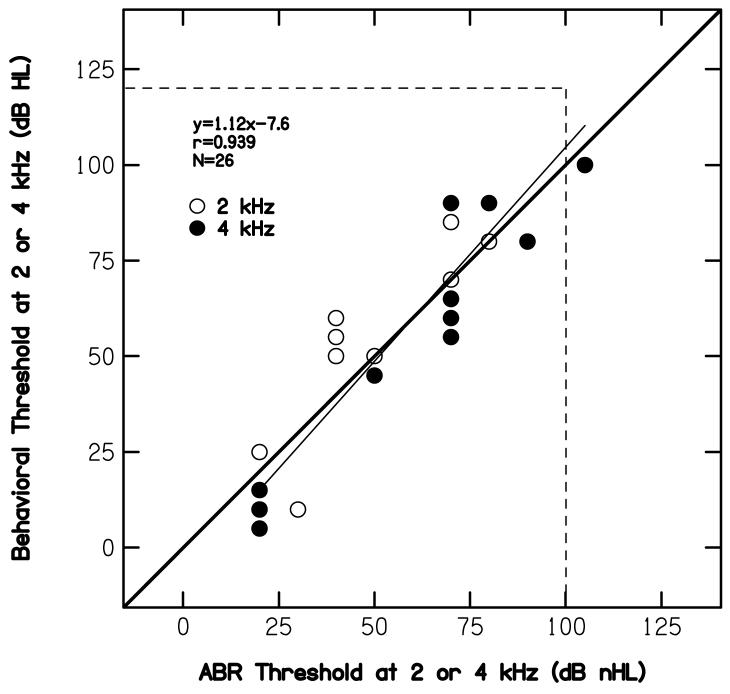
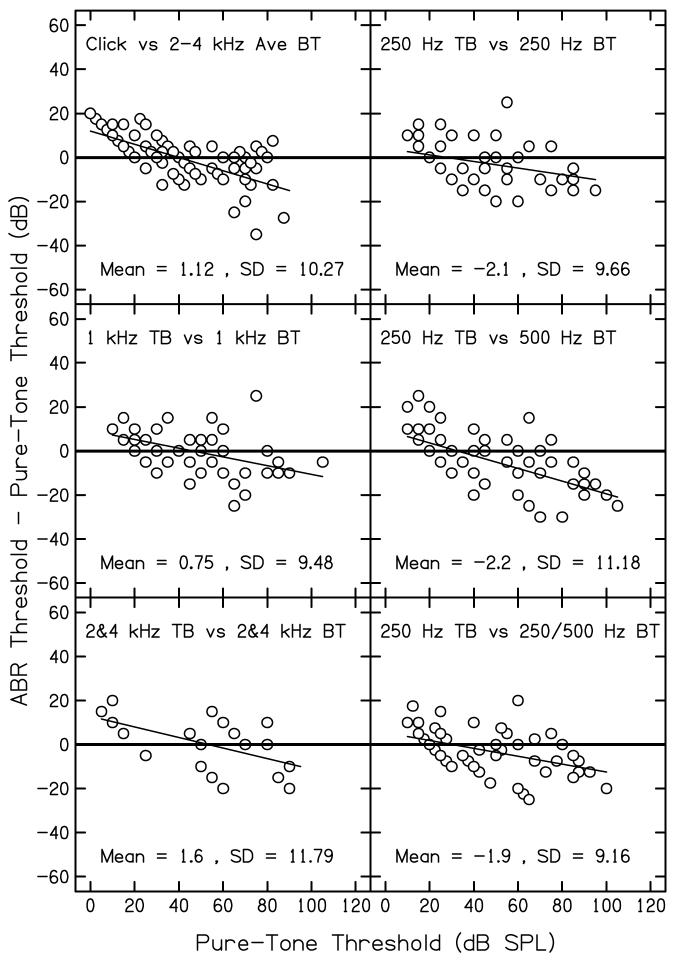
Results: Correlation was 0.94 between click-evoked ABR thresholds and the average pure-tone threshold at 2 and 4 kHz. Correlations exceeded 0.92 between ABR thresholds for the 250-Hz tone burst and low-frequency behavioral thresholds (250 Hz, 500 Hz, and the average pure-tone thresholds at 250 and 500 Hz). Similar or higher correlations were observed when ABR thresholds at other frequencies were compared with the pure-tone thresholds at corresponding frequencies. Differences between ABR and behavioral threshold depended on behavioral threshold, with ABR thresholds overestimating behavioral threshold in cases of normal hearing and underestimating behavioral threshold in cases of hearing loss.
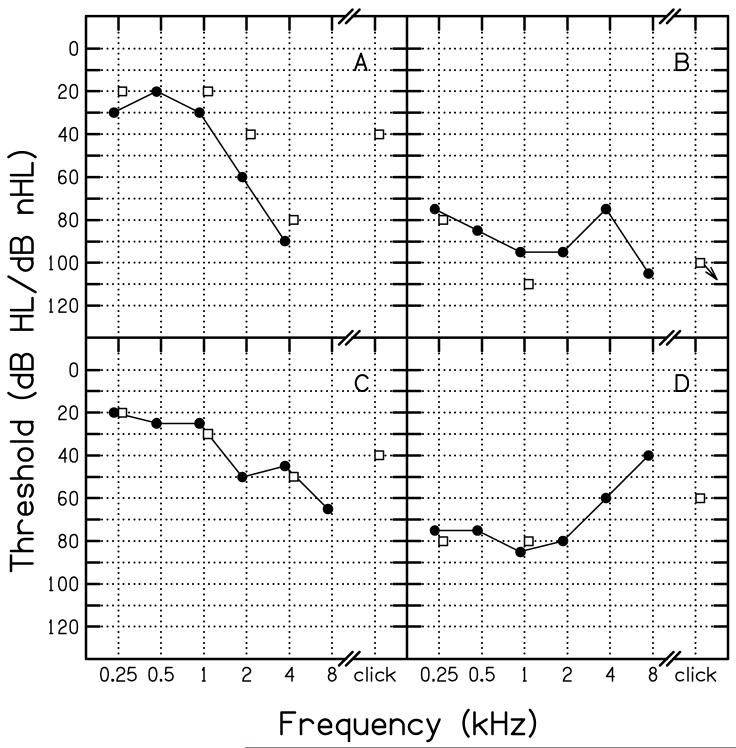
Conclusions: These results suggest that ABR thresholds can be used to predict pure-tone behavioral thresholds for a wide range of frequencies. Although controversial, the data reviewed in this paper suggest that click-evoked ABR thresholds result in reasonable predictions of the average behavioral thresholds at 2 and 4 kHz. However, there were cases for which click-evoked ABR thresholds underestimated hearing loss at these frequencies. There are several other reasons why click-evoked ABR measurements were made, including that they (1) generally result in well-formed responses, (2) assist in determining whether auditory neuropathy exists, and (3) can be obtained in a relatively brief amount of time. Low-frequency thresholds were predicted well by ABR thresholds to a single-cycle, 250-Hz tone burst. In combination, click-evoked and low-frequency tone burst-evoked ABR threshold measurements might be used to quickly provide important clinical information for both ends of the audiogram. These measurements could be supplemented by ABR threshold measurements at other frequencies, if time permits. However, it may be possible to plan initial intervention strategies based on data for these two stimuli.
Figures
References
-
- American National Standards Institute (ANSI) Specifications for audiometers, S3.6. New York, NY: 1996.
-
- Berlin CI, Hood L, Morlet T, Rose K, Brashears S. Auditory neuropathy/dys-synchrony: Diagnosis and management. Men. Ret. Devel. Dis. Res. Rev. 2003;9:225–231. - PubMed
-
- Don M, Eggermont JJ. Analysis of the click-evoked brainstem potentials using high-pass noise masking. J. Acoust. Soc. Am. 1978;63:1084–1092. - PubMed
-
- Don M, Eggermont JJ, Brackmann DE. Reconstruction of the audiogram using brain stem responses and high-pass noise masking. Ann. Otol. Rhinol, Laryngol. 1979;83(Suppl 57):1–20. - PubMed
-
- Don M, Masuda A, Nelson R, Brackmann D. Successful detection of small acoustic tumors using the stacked derived-band auditory brainstem response amplitude. Am. J. Otol. 1997;18:608–621. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
