

Determining effective methadone doses for individual opioid-dependent patients
- PMID: 16448216
- PMCID: PMC1360079
- DOI: 10.1371/journal.pmed.0030080
Determining effective methadone doses for individual opioid-dependent patients
Abstract
Background: Randomized clinical trials of methadone maintenance have found that on average high daily doses are more effective for reducing heroin use, and clinical practice guidelines recommend 60 mg/d as a minimum dosage. Nevertheless, many clinicians report that some patients can be stably maintained on lower methadone dosages to optimal effect, and clinic dosing practices vary substantially. Studies of individual responses to methadone treatment may be more easily translated into clinical practice.
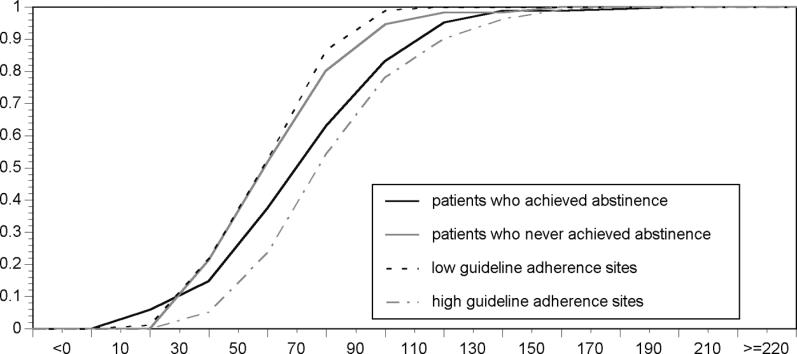
Methods and findings: A volunteer sample of 222 opioid-dependent US veterans initiating methadone treatment was prospectively observed over the year after treatment entry. In the 168 who achieved at least 1 mo of heroin abstinence, methadone dosages on which patients maintained heroin-free urine samples ranged from 1.5 mg to 191.2 mg (median = 69 mg). Among patients who achieved heroin abstinence, higher methadone dosages were predicted by having a diagnosis of posttraumatic stress disorder or depression, having a greater number of previous opioid detoxifications, living in a region with lower average heroin purity, attending a clinic where counselors discourage dosage reductions, and staying in treatment longer. These factors predicted 42% of the variance in dosage associated with heroin abstinence.
Conclusions: Effective and ineffective methadone dosages overlap substantially. Dosing guidelines should focus more heavily on appropriate processes of dosage determination rather than solely specifying recommended dosages. To optimize therapy, methadone dosages must be titrated until heroin abstinence is achieved.
Conflict of interest statement
Figures
Similar articles
-
High-dose methadone produces superior opioid blockade and comparable withdrawal suppression to lower doses in opioid-dependent humans.Psychopharmacology (Berl). 2002 May;161(2):202-12. doi: 10.1007/s00213-002-1027-0. Epub 2002 Mar 13. Psychopharmacology (Berl). 2002. PMID: 11981600
-
Methadone maintenance treatment (MMT): a review of historical and clinical issues.Mt Sinai J Med. 2000 Oct-Nov;67(5-6):347-64. Mt Sinai J Med. 2000. PMID: 11064485 Review.
-
Methadone doses of 100 mg or greater are more effective than lower doses at suppressing heroin self-administration in opioid-dependent volunteers.Addiction. 2005 Oct;100(10):1496-509. doi: 10.1111/j.1360-0443.2005.01232.x. Addiction. 2005. PMID: 16185211 Clinical Trial.
-
Dosage regimes in the prescription of heroin and other narcotics to chronic opioid addicts in Switzerland--Swiss national cohort study.Eur Addict Res. 2004;10(1):41-8. doi: 10.1159/000073725. Eur Addict Res. 2004. PMID: 14665805
-
Neurobiology of addictive behaviors and its relationship to methadone maintenance.Mt Sinai J Med. 2000 Oct-Nov;67(5-6):375-80. Mt Sinai J Med. 2000. PMID: 11064487 Review.
Cited by
-
Trauma and post-traumatic stress disorder in patients treated for opioid use disorder: findings from a 12-month cohort study.BJPsych Open. 2021 Jul 22;7(4):e138. doi: 10.1192/bjo.2021.971. BJPsych Open. 2021. PMID: 36043687 Free PMC article.
-
Association between rs1799971 in the mu opioid receptor gene and methadone maintenance treatment response.J Clin Lab Anal. 2022 Nov;36(11):e24750. doi: 10.1002/jcla.24750. Epub 2022 Oct 28. J Clin Lab Anal. 2022. PMID: 36305091 Free PMC article.
-
Adverse Events During Treatment Induction With Injectable Diacetylmorphine and Hydromorphone for Opioid Use Disorder.J Addict Med. 2019 Sep/Oct;13(5):354-361. doi: 10.1097/ADM.0000000000000505. J Addict Med. 2019. PMID: 30747750 Free PMC article.
-
The newer Opioid Agonist Treatment with lower substitutive opiate doses is associated with better toxicology outcome than the older Harm Reduction Treatment.Ann Gen Psychiatry. 2016 Nov 25;15:34. doi: 10.1186/s12991-016-0109-z. eCollection 2016. Ann Gen Psychiatry. 2016. PMID: 27933094 Free PMC article.
-
The Prevalence and Psychosocial Correlates of Ketum (Mitragyna speciosa) Use among Individuals on Methadone Maintenance Therapy Programme in Hospital Taiping, Malaysia.Healthcare (Basel). 2022 Apr 17;10(4):746. doi: 10.3390/healthcare10040746. Healthcare (Basel). 2022. PMID: 35455923 Free PMC article.
References
-
- Kosten TR, Schottenfeld R, Ziedonis D, Falcioni J. Buprenorphine versus methadone maintenance for opioid dependence. J Nerv Ment Dis. 1993;181:358–364. - PubMed
-
- Strain EC, Stitzer ML, Liebson IA, Bigelow GE. Methadone dose and treatment outcome. Drug Alcohol Depend. 1993;33:105–117. - PubMed
-
- Ling W, Wesson DR, Charuvastra C, Klett CJ. A controlled trial comparing buprenorphine and methadone maintenance in opioid dependence. Arch Gen Psychiatry. 1996;53:401–407. - PubMed
-
- Maxwell S, Shinderman M. Optimizing response to methadone maintenance treatment: Use of higher dose methadone. J Psychoactive Drugs 1999. 1999;31:95–102. - PubMed
-
- US Department of Veterans Affairs. Management of substance use disorders in primary and specialty care, v 1.0. 2001 Available: http://www.oqp.med.va.gov/cpg/SUD/SUD_Base.htm. Accessed 6 April 2004.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
