

A meta-analysis of hyperfractionated and accelerated radiotherapy and combined chemotherapy and radiotherapy regimens in unresected locally advanced squamous cell carcinoma of the head and neck
- PMID: 16448551
- PMCID: PMC1379652
- DOI: 10.1186/1471-2407-6-28
A meta-analysis of hyperfractionated and accelerated radiotherapy and combined chemotherapy and radiotherapy regimens in unresected locally advanced squamous cell carcinoma of the head and neck
Abstract
Background: Former meta-analyses have shown a survival benefit for the addition of chemotherapy (CHX) to radiotherapy (RT) and to some extent also for the use of hyperfractionated radiation therapy (HFRT) and accelerated radiation therapy (AFRT) in locally advanced squamous cell carcinoma (SCC) of the head and neck. However, the publication of new studies and the fact that many older studies that were included in these former meta-analyses used obsolete radiation doses, CHX schedules or study designs prompted us to carry out a new analysis using strict inclusion criteria.
Methods: Randomised trials testing curatively intended RT (> or =60 Gy in >4 weeks/>50 Gy in <4 weeks) on SCC of the oral cavity, oropharynx, hypopharynx, and larynx published as full paper or in abstract form between 1975 and 2003 were eligible. Trials comparing RT alone with concurrent or alternating chemoradiation (5-fluorouracil (5-FU), cisplatin, carboplatin, mitomycin C) were analyzed according to the employed radiation schedule and the used CHX regimen. Studies comparing conventionally fractionated radiotherapy (CFRT) with either HFRT or AFRT without CHX were separately examined. End point of the meta-analysis was overall survival.
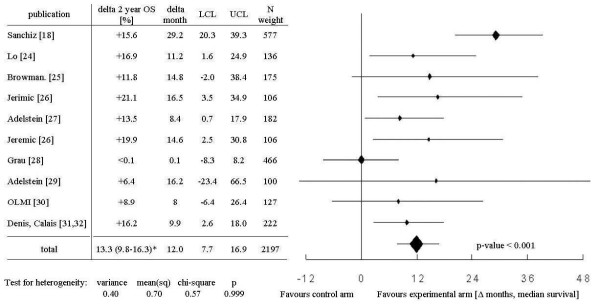
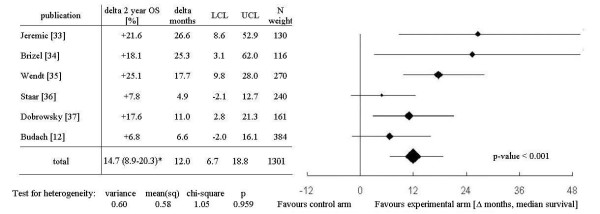
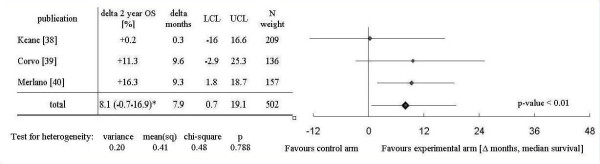
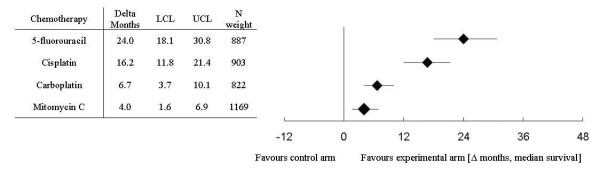
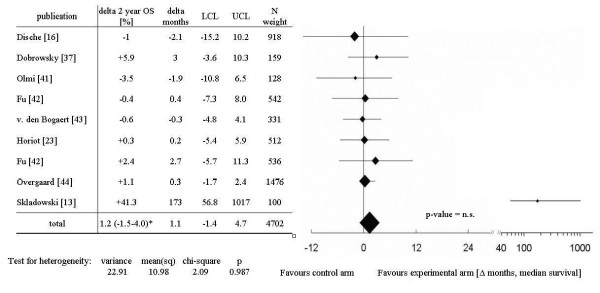
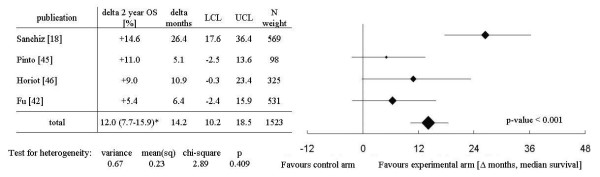
Results: Thirty-two trials with a total of 10 225 patients were included into the meta-analysis. An overall survival benefit of 12.0 months was observed for the addition of simultaneous CHX to either CFRT or HFRT/AFRT (p < 0.001). Separate analyses by cytostatic drug indicate a prolongation of survival of 24.0 months, 16.8 months, 6.7 months, and 4.0 months, respectively, for the simultaneous administration of 5-FU, cisplatin-based, carboplatin-based, and mitomycin C-based CHX to RT (each p < 0.01). Whereas no significant gain in overall survival was observed for AFRT in comparison to CFRT, a substantial prolongation of median survival (14.2 months, p < 0.001) was seen for HFRT compared to CFRT (both without CHX).
Conclusion: RT combined with simultaneous 5-FU, cisplatin, carboplatin, and mitomycin C as single drug or combinations of 5-FU with one of the other drugs results in a large survival advantage irrespective the employed radiation schedule. If radiation therapy is used as single modality, hyperfractionation leads to a significant improvement of overall survival. Accelerated radiation therapy alone, especially when given as split course radiation schedule or extremely accelerated treatments with decreased total dose, does not increase overall survival.
Figures
References
-
- Pignon JP, Bourhis J, Domenge C, Designe L. Chemotherapy added to locoregional treatment for head and neck squamous-cell carcinoma: three meta-analyses of updated individual data. MACH-NC Collaborative Group. Meta-Analysis of Chemotherapy on Head and Neck Cancer. Lancet. 2000;355:949–55. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
