

Surgery for non-small cell lung cancer: systematic review and meta-analysis of randomised controlled trials
- PMID: 16449262
- PMCID: PMC2104670
- DOI: 10.1136/thx.2005.051995
Surgery for non-small cell lung cancer: systematic review and meta-analysis of randomised controlled trials
Abstract
Background: Surgery is considered the treatment of choice for patients with resectable stage I and II (and some patients with stage IIIA) non-small cell lung cancer (NSCLC), but there have been no previously published systematic reviews.
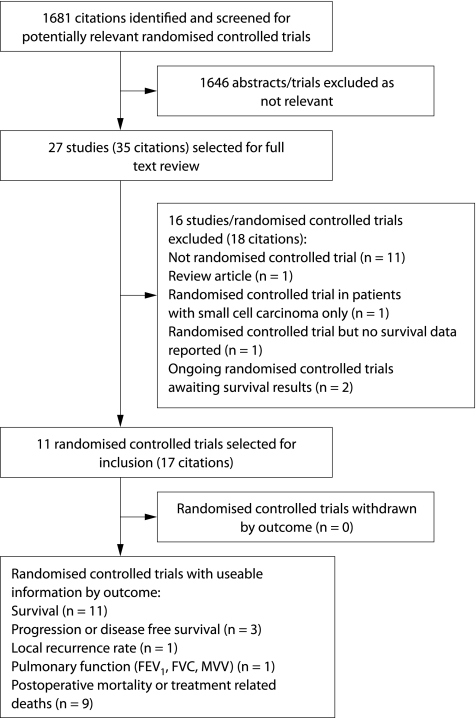
Methods: A systematic review and meta-analysis of randomised controlled trials was conducted to determine whether surgical resection improves disease specific mortality in patients with stages I-IIIA NSCLC compared with non-surgical treatment, and to compare the efficacy of different surgical approaches.
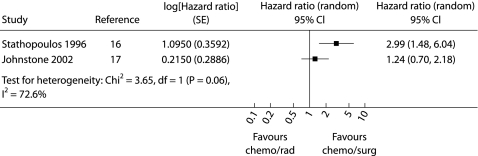
Results: Eleven trials were included. No studies had untreated control groups. In a pooled analysis of three trials, 4 year survival was superior in patients undergoing resection with stage I-IIIA NSCLC who had complete mediastinal lymph node dissection compared with lymph node sampling (hazard ratio estimated at 0.78 (95% CI 0.65 to 0.93)). Another trial reported an increased rate of local recurrence in patients with stage I NSCLC treated with limited resection compared with lobectomy. One small study reported a survival advantage among patients with stage IIIA NSCLC treated with chemotherapy followed by surgery compared with chemotherapy followed by radiotherapy. No other trials reported significant improvements in survival after surgery compared with non-surgical treatment.
Conclusion: It is difficult to draw conclusions about the efficacy of surgery for locoregional NSCLC because of the small number of participants studied and methodological weaknesses of the trials. However, current evidence suggests that complete mediastinal lymph node dissection is associated with improved survival compared with node sampling in patients with stage I-IIIA NSCLC undergoing resection.
Conflict of interest statement
Competing interests: none.

Comment in
-
When in doubt should we cut it out? The role of surgery in non-small cell lung cancer.Thorax. 2006 Jul;61(7):554-6. doi: 10.1136/thx.2006.060558. Thorax. 2006. PMID: 16807388 Free PMC article.
-
When in doubt should we cut it out? The role of surgery in non-small-cell lung cancer.Thorax. 2007 Feb;62(2):190-1; author reply 191. Thorax. 2007. PMID: 17287308 Free PMC article. No abstract available.
References
-
- Reif M, Socinski M A, Rivera M P. Evidence‐based medicine in the treatment of non‐small cell lung cancer. Clin Chest Med 200021107–120. - PubMed
-
- Scott W, Howington J, Movsas B. Treatment of stage II non‐small cell lung cancer. Chest 2003123(Suppl 1)188–201S. - PubMed
-
- Smythe W. Treatment of stage I non‐small cell lung carcinoma. Chest 2003123(Suppl 1)181–7S. - PubMed
-
- Flehinger B J, Kimmel M, Melamed M R. The effect of surgical treatment on survival from early lung cancer. Implications for screening. Chest 19921011013–1018. - PubMed
-
- Sobue T, Suzuki T, Matsuda M.et al Survival for clinical stage I lung cancer not surgically treated: comparison between screen‐detected and symptom‐detected cases. Cancer 199269685–692. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical