

Outcome of acute fulminant myocarditis in children
- PMID: 16449512
- PMCID: PMC1861180
- DOI: 10.1136/hrt.2005.078402
Outcome of acute fulminant myocarditis in children
Abstract
Objectives: To highlight clinical features and outcome of acute fulminant myocarditis (AFM) in children.
Methods: Diagnostic criteria were (1) the presence of severe and acute heart failure; (2) left ventricular dysfunction on echocardiography; (3) recent history of viral illness; and (4) no history of cardiomyopathy.
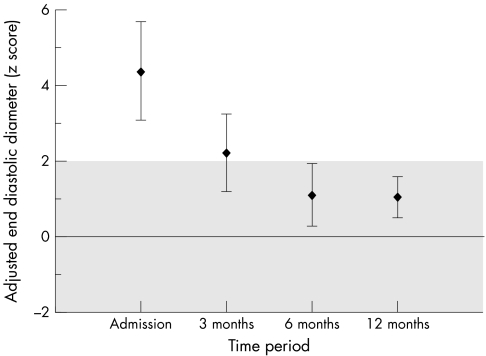
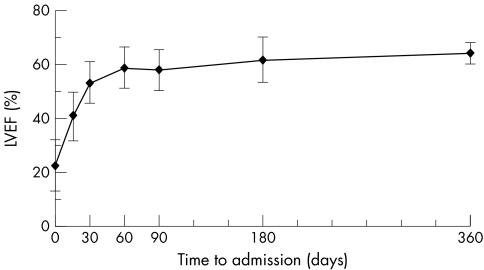
Results: Eleven children were included between 1998 and 2003, at a median age of 1 (0 to 9) year. Their mean left ventricular ejection fraction (LVEF) was 22 (SD 9)% at presentation. A virus was identified in five patients: human parvovirus B19 (n = 2), Epstein-Barr (n = 1), varicella zoster (n = 1), and coxsackie (n = 1). The median intensive care unit course was 13 (2-34) days. Intravenous inotropic support was required by nine patients and eight were mechanically ventilated. All patients received corticosteroid, associated with intravenous immunoglobulin in seven. Five patients experienced cardiocirculatory arrest that was successfully resuscitated in four. At a median follow up of 58.7 (33.8-83.1) months, the 10 survivors are asymptomatic with normalised LVEF.
Conclusion: Despite a severe presentation, the outcome of AFM is favourable. Aggressive symptomatic management is warranted and heart transplantation should be considered only when maximal supportive therapy does not lead to improvement.
Conflict of interest statement
Competing interests: None declared.
References
-
- Feldman A M, McNamara D. Myocarditis. N Engl J Med 20003431388–1398. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous