

Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006: diagnosis and management
- PMID: 16450016
- PMCID: PMC2538984
- DOI: 10.1016/s0828-282x(06)70237-9
Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006: diagnosis and management
Erratum in
- Can J Cardiol. 2006 Mar 1;22(3):271
Abstract
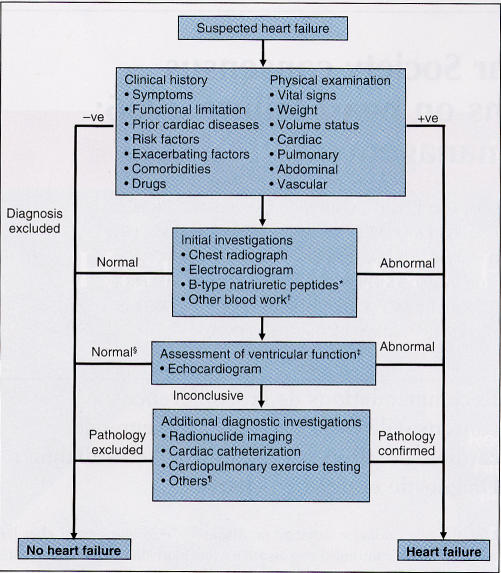
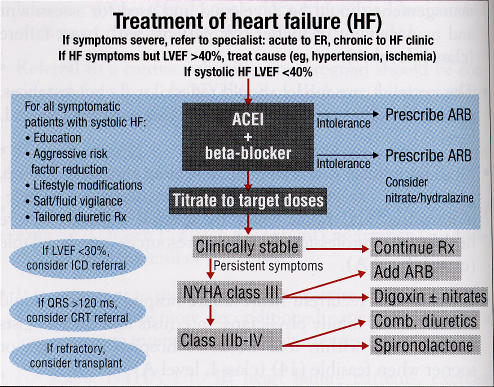
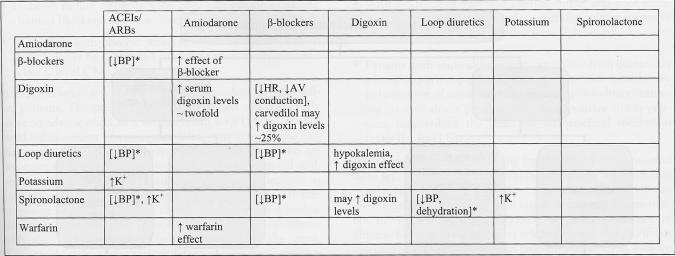
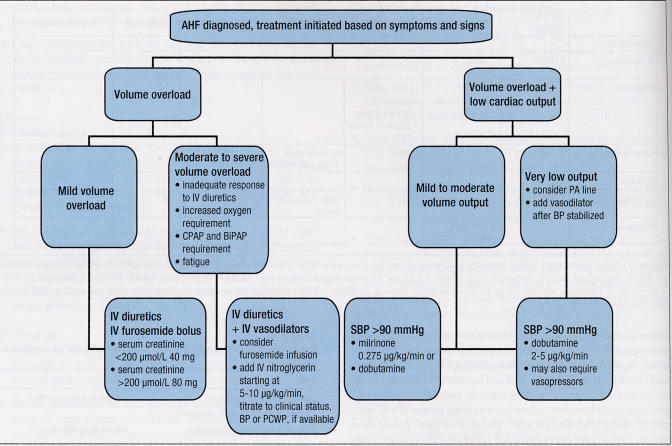
Heart failure remains a common diagnosis, especially in older individuals. It continues to be associated with significant morbidity and mortality, but major advances in both diagnosis and management have occurred and will continue to improve symptoms and other outcomes in patients. The Canadian Cardiovascular Society published its first consensus conference recommendations on the diagnosis and management of heart failure in 1994, followed by two brief updates, and reconvened this consensus conference to provide a comprehensive review of current knowledge and management strategies. New clinical trial evidence and meta-analyses were critically reviewed by a multidisciplinary primary panel who developed both recommendations and practical tips, which were reviewed by a secondary panel. The resulting document is intended to provide practical advice for specialists, family physicians, nurses, pharmacists and others who are involved in the care of heart failure patients. Management of heart failure begins with an accurate diagnosis, and requires rational combination drug therapy, individualization of care for each patient (based on their symptoms, clinical presentation and disease severity), appropriate mechanical interventions including revascularization and devices, collaborative efforts among health care professionals, and education and cooperation of the patient and their immediate caregivers. The goal is to translate best evidence-based therapies into clinical practice with a measureable impact on the health of heart failure patients in Canada.
L’insuffisance cardiaque demeure un diagnostic répandu, surtout chez les sujets âgés. Elle continue d’être associée à une morbidité et à une mortalité importantes, mais de grands progrès ont été accomplis sur les plans du diagnostic et de la prise en charge de la maladie et ils amélioreront encore les symptômes et le pronostic des patients. C’est en 1994 que la Société canadienne de cardiologie a publié son premier rapport consensuel sur le diagnostic et la prise en charge de l’insuffisance cardiaque, suivi de brèves mises à jour; et elle a choisi de répéter l’exercice afin de faire le point de manière globale sur les connaissances et les stratégies thérapeutiques actuelles.
Les conclusions et méta-analyses d’essais cliniques récents ont été analysées par un comité principal pluridisciplinaire qui a formulé ses recommandations et ses conseils pratiques avant de les soumettre à un second comité. Le document qui en résulte vise à guider de manière concrète les spécialistes, médecins de famille, infirmières, pharmaciens et autres intervenants appelés à soigner les insuffisants cardiaques.
La prise en charge de l’insuffisance cardiaque commence par un diagnostic juste et repose sur l’administration de traitements pharmacologiques associatifs, sur une individualisation de l’approche thérapeutique (selon les symptômes, le tableau clinique et la gravité de chaque cas), sur des interventions de type mécanique appropriées, telles que l’angioplastie ou d’autres dispositifs, sur une approche pluridisciplinaire concertée et sur l’enseignement au patient et à ses aidants naturels, pour une meilleure coopération. L’objectif est de transposer dans la pratique clinique les meilleurs traitements issus de la recherche, éprouvés et susceptibles d’exercer un impact véritable sur la santé des insuffisants cardiaques au Canada.
Figures
References
-
- Johansen H, Strauss B, Arnold JMO, Moe G, Liu P. On the rise: The current and projected future burden of congestive heart failure hospitalization in Canada. Can J Cardiol. 2003;19:430–5. - PubMed
-
- Johnstone DE, Abdulla A, Arnold JMO, et al. Report of the Canadian Cardiovascular Society’s Consensus Conference on the diagnosis and management of heart failure. Can J Cardiol. 1994;10:613–31. - PubMed
-
- Liu P, Arnold JMO, Belenkie I, et al. The 2001 Canadian Cardiovascular Society consensus guideline update for the management and prevention of heart failure. Can J Cardiol. 2001;17(Suppl E):5E–25E. - PubMed
-
- Liu P, Arnold JMO, Belenkie I, et al. The 2002/3 Canadian Cardiovascular Society consensus guideline update for the diagnosis and management of heart failure. Can J Cardiol. 2003;19:347–56. - PubMed
-
- Maisel AS, Krishnaswamy P, Nowak RM, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;347:161–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
