

Mechanisms of progression and regression of renal lesions of chronic nephropathies and diabetes
- PMID: 16453013
- PMCID: PMC1359063
- DOI: 10.1172/JCI27699
Mechanisms of progression and regression of renal lesions of chronic nephropathies and diabetes
Abstract
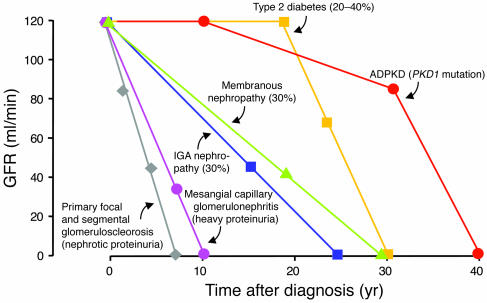
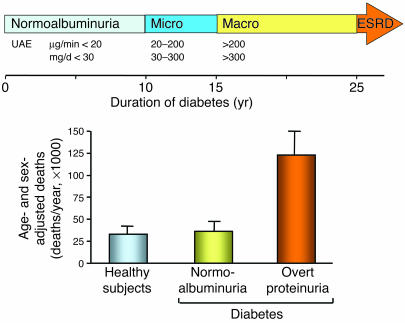
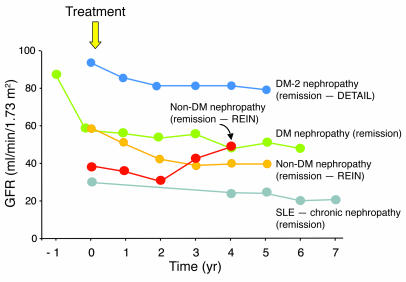
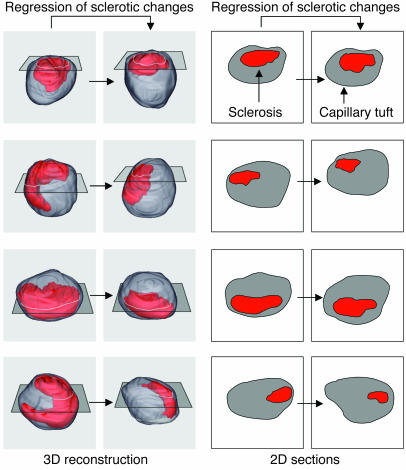
The incidence of chronic kidney diseases is increasing worldwide, and these conditions are emerging as a major public health problem. While genetic factors contribute to susceptibility and progression of renal disease, proteinuria has been claimed as an independent predictor of outcome. Reduction of urinary protein levels by various medications and a low-protein diet limits renal function decline in individuals with nondiabetic and diabetic nephropathies to the point that remission of the disease and regression of renal lesions have been observed in experimental animals and even in humans. In animal models, regression of glomerular structural changes is associated with remodeling of the glomerular architecture. Instrumental to this discovery were 3D reconstruction studies of the glomerular capillary tuft, which allowed the quantification of sclerosis volume reduction and capillary regeneration upon treatment. Regeneration of capillary segments might result from the contribution of resident cells, but progenitor cells of renal or extrarenal origin may also have a role. This review describes recent advances in our understanding of the mechanisms and mediators underlying renal tissue repair ultimately responsible for regression of renal injury.
Figures
References
-
- Bright, R. 1827. Report of medical cases, selected with a view of illustrating the symptoms and cure of diseases by a reference to morbid anatomy. Longman, Rees, Orme, Brown & Green. London, United Kingdom. 724 pp.
-
- Addis, T., and Oliver, J. 1931. The renal lesion in Bright’s disease. P.B. Hoeber. New York, New York, USA. 628 pp.
-
- Addis T. The osmotic work of the kidney and the treatment of glomerular nephritis. Trans. Assoc. Am. Phys. 1940;55:223–229.
-
- Chanutin A, Ferris EB. Experimental renal insufficiency produced by partial nephrectomy. 1. Control diet. Arch. Intern. Med. 1932;49:767–787.
-
- Volhard, F., and Fahr, T.H. 1914. Die Bright’sche Nierenkrankheit [In German]. Julius Springer. Berlin, Germany. 292 pp.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
