

Oral misoprostol for induction of labour at term: randomised controlled trial
- PMID: 16455695
- PMCID: PMC1388124
- DOI: 10.1136/bmj.38729.513819.63
Oral misoprostol for induction of labour at term: randomised controlled trial
Abstract
Objective: To compare oral misoprostol solution with vaginal prostaglandin gel (dinoprostone) for induction of labour at term to determine whether misoprostol is superior.
Design: Randomised double blind placebo controlled trial.
Setting: Maternity departments in three hospitals in Australia. Population Pregnant women with a singleton cephalic presentation at > or = 36+6 weeks' gestation, with an indication for prostaglandin induction of labour.
Interventions: 20 mug oral misoprostol solution at ourly intervals and placebo vaginal gel or vaginal dinoprostone gel at six hourly intervals and placebo oral solution.
Main outcome measures: Vaginal birth within 24 hours; uterine hyperstimulation with associated changes in fetal heart rate; caesarean section (all); and caesarean section for fetal distress.
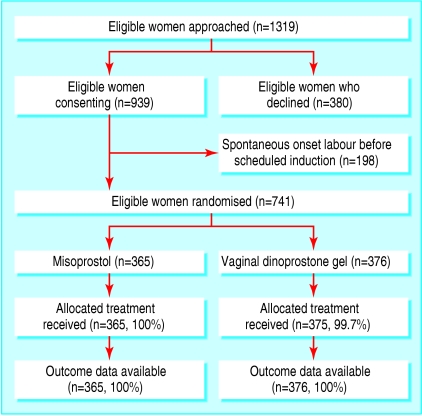
Results: 741 women were randomised, 365 to the misoprostol group and 376 to the vaginal dinoprostone group. There were no significant differences between the two treatment groups in the primary outcomes: vaginal birth not achieved in 24 hours (misoprostol 168/365 (46.0%) v dinoprostone 155/376 (41.2%); relative risk 1.12, 95% confidence interval 0.95 to 1.32; P = 0.134), caesarean section (83/365 (22.7%) v 100/376 (26.6%); 0.82, 0.64 to 1.06; P = 0.127), caesarean section for fetal distress (32/365 (8.8%) v 35/376 (9.3%); 0.91, 0.57 to 1.44; P = 0.679), or uterine hyperstimulation with changes in fetal heart rate (3/365 (0.8%) v 6/376 (1.6%); 0.55, 0.14 to 2.21; P = 0.401). Although there were differences in the process of labour induction, there were no significant differences in adverse maternal or neonatal outcomes.
Conclusions: This trial shows no evidence that oral misoprostol is superior to vaginal dinoprostone for induction of labour. However, it does not lead to poorer health outcomes for women or their infants, and oral treatment is preferred by women.
Trial registration: National Health and Medical Research Council, Perinatal Trials, PT0361.
References
-
- Riskin-Mashiah S, Wilkins I. Cervical ripening. Obstet Gynecol Clin North Am 1999;26: 243-57. - PubMed
-
- Laws PJ, Sullivan EA. Australia's mothers and babies 2002. Sydney: Australian Institute of Health and Welfare (AIHW), National Perinatal Statistics Unit (NPSU). 2004.
-
- Nassar N, Sullivan EA, Lancaster P, Day P. Australia's mothers and babies 1998. Sydney: AIHW National Perinatal Statistics Unit, 2000.
-
- Garris RE, Kirkwood CF. Misoprostol: a prostaglandin E1 analogue. Clin Pharm 1989;8: 627-44. - PubMed
-
- Collins PW, Pappo R, Dajani EZ. Chemistry and synthetic development of misoprostol. Dig Dis Sci 1985;30: 114-7S. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources