

Diagnosis and conservative treatment of tubercular rectoprostatic fistula
- PMID: 16460634
- PMCID: PMC1963633
- DOI: 10.1308/147870806x83242
Diagnosis and conservative treatment of tubercular rectoprostatic fistula
Abstract
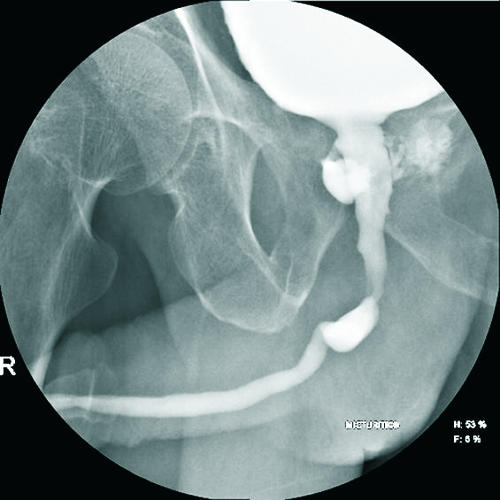
Objective: To present our experience with three cases of rectoprostatic fistula with special emphasis on diagnosis and conservative management.
Patients and methods: Three middle-aged men presented to us differently. All had spontaneous rectoprostatic fistulas. Biopsy showed tuberculosis though three consecutive urine samples for acid-fast bacilli were negative. None of the patients were immunocompromised. Their upper tracts were normal and all had a past history of pulmonary tuberculosis. They were started on antitubercular drugs and urinary diversion with or without faecal diversion.
Results: All fistulae healed completely within 6 weeks of starting antitubercular treatment. One patient healed with bladder neck stenosis that required bladder neck incision. Voiding was normal on 1-year follow-up.
Conclusion: Spontaneous tubercular rectoprostatic fistulae are rare. There should be a strong clinical suspicion in endemic areas. Prostatic biopsy proves the diagnosis. Conservative management with antitubercular drugs and urinary diversion with or without faecal diversion has a high success rate and should be the first line of treatment even if urine is negative for acid-fast bacilli.
Figures



References
-
- Mondal A, Ghosh E, Ghose A. The role of transrectal fine needle aspiration cytology in the diagnosis of prostatic nodules suspicious of malignancy – a study of 126 cases. Ind J Pathol Microbiol. 1990;33:23. - PubMed
-
- Stamler JS, Bauer JJ, Janonitz HD. Rectourethroperineal fistula in Crohn's disease. Am J Gastroenterol. 1985;80:111–2. - PubMed
-
- Veenema RJ, Lattimer JK. Genital tuberculosis in the male: clinical pathology and effect on fertility. J Urol. 1957;78:65–77. - PubMed
-
- Culp OS, Calhoo HW. A variety of rectourethral fistulas: experience with twenty cases. J Urol. 1964;91:560–71. - PubMed
-
- Symes JM, Blandy JP. Tuberculosis of the male urethra. Br J Urol. 1973;45:432–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous