

Description of 12 cases of nephrogenic fibrosing dermopathy and review of the literature
- PMID: 16461069
- PMCID: PMC1434722
- DOI: 10.1016/j.semarthrit.2005.08.002
Description of 12 cases of nephrogenic fibrosing dermopathy and review of the literature
Abstract
Objectives: To review the clinical and laboratory features of 12 cases of nephrogenic fibrosing dermopathy (NFD) studied at our institution and of 70 previously described cases in the literature.
Methods: Clinical evaluation and laboratory studies of 12 patients with NFD associated with chronic hemodialysis or peritoneal dialysis for end-stage renal disease and a review of 23 previous publications describing 70 patients with this disease.
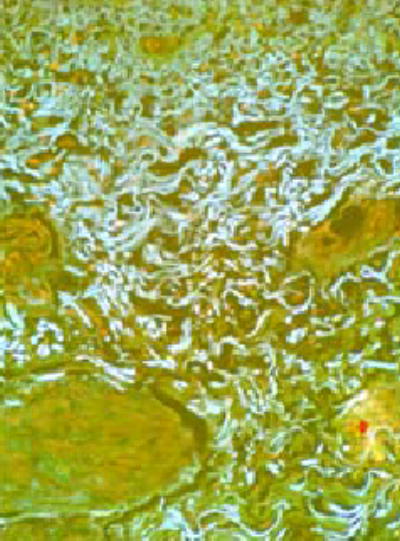
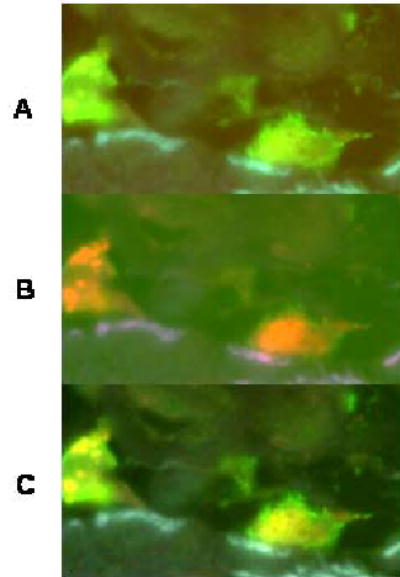
Results: Eleven patients undergoing chronic hemodialysis and 1 patient undergoing chronic peritoneal dialysis for end-stage renal failure developed a severe and progressive cutaneous fibrotic process with woody induration of legs, thighs, hands, and forearms, and severe loss of motion and flexion contractures in multiple joints. Several patients displayed systemic involvement including fibrosis of muscles, myocardium, and lungs and marked elevations of the erythrocyte sedimentation rate and/or C-reactive protein. Three patients died within 2 years of symptom onset. A review of previously published reports of this disorder confirmed the presence of systemic involvement and a poor prognosis with a high mortality rate.
Conclusions: NFD is a severe and usually progressive systemic fibrotic disease affecting the dermis, subcutaneous fascia, and striated muscles. It also appears that the disease can cause fibrosis of lungs, myocardium, and other organs.
Figures








Comment in
-
Nephrogenic fibrosing dermopathy/nephrogenic systemic fibrosis--setting the record straight.Semin Arthritis Rheum. 2006 Feb;35(4):208-10. doi: 10.1016/j.semarthrit.2005.09.005. Semin Arthritis Rheum. 2006. PMID: 16461067 No abstract available.
References
-
- Cowper SE, Robin HS, Steinberg SM, Su LD, Gupta S, LeBoit PE. Scleromyxoedema-like cutaneous disease in renal-dialysis patients. Lancet. 2000;356:1000–01. - PubMed
-
- Cowper SE, Su LD, Bhawan J, Robin HS, LeBoit PE. Nephrogenic fibrosing dermopathy. Am J Dermatopathol. 2001;23:383–93. - PubMed
-
- http://www.icnfdr.org/ Accessed June 9, 2005.
-
- Ting WW, Stone MS, Madison KC, Kurtz K. Nephrogenic fibrosing dermopathy with systemic involvement. Arch Dermatol. 2003;139:903–06. - PubMed
-
- Jimenez SA, Arlett CM, Sandorfi N, Derk C, Latinis K, Sawaya H, et al. Dialysis-Associated Systemic Fibrosis (Nephrogenic Fibrosing Dermopathy) Arthritis Rheum. 2004;50:2660–66. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
