

JPN Guidelines for the management of acute pancreatitis: diagnostic criteria for acute pancreatitis
- PMID: 16463208
- PMCID: PMC2779365
- DOI: 10.1007/s00534-005-1048-2
JPN Guidelines for the management of acute pancreatitis: diagnostic criteria for acute pancreatitis
Abstract
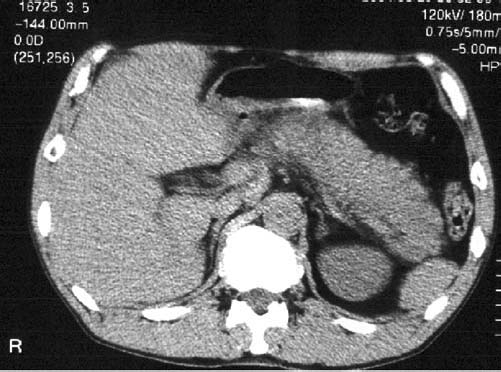
The currently used diagnostic criteria for acute pancreatitis in Japan are presentation with at least two of the following three manifestations: (1) acute abdominal pain and tenderness in the upper abdomen; (2) elevated levels of pancreatic enzyme in the blood, urine, or ascitic fluid; and (3) abnormal imaging findings in the pancreas associated with acute pancreatitis. When a diagnosis is made on this basis, other pancreatic diseases and acute abdomen can be ruled out. The purpose of this article is to review the conventional criteria and, in particular, the various methods of diagnosis based on pancreatic enzyme values, with the aim of improving the quality of diagnosis of acute pancreatitis and formulating common internationally agreed criteria. The review considers the following recommendations: Better even than the total blood amylase level, the blood lipase level is the best pancreatic enzyme for the diagnosis of acute pancreatitis and its differentiation from other diseases. A pivotal factor in the diagnosis of acute pancreatitis is identifying an increase in pancreatic enzymes in the blood. Ultrasonography (US) is also one of the procedures that should be performed in all patients with suspected acute pancreatitis. Magnetic resonance imaging (MRI) is one of the most important imaging procedures for diagnosing acute pancreatitis and its intraperitoneal complications. Computed tomography (CT) is also one of the most important imaging procedures for diagnosing acute pancreatitis and its intraabdominal complications. CT should be performed when a diagnosis of acute pancreatitis cannot be established on the basis of the clinical findings, results of blood and urine tests, or US, or when the etiology of the pancreatitis is unknown. When acute pancreatitis is suspected, chest and abdominal X-ray examinations should be performed to determine whether any abnormal findings caused by acute pancreatitis are present. Because the etiology of acute pancreatitis can have a crucial influence on both the treatment policy and severity assessment, it should be evaluated promptly and accurately. It is particularly important to differentiate between gallstone-induced acute pancreatitis, which requires treatment of the biliary system, and alcohol-induced acute pancreatitis, which requires a different form of treatment.
Figures


Similar articles
-
New diagnostic criteria of acute pancreatitis.J Hepatobiliary Pancreat Sci. 2010 Jan;17(1):24-36. doi: 10.1007/s00534-009-0214-3. Epub 2009 Dec 11. J Hepatobiliary Pancreat Sci. 2010. PMID: 20012328
-
Serum amylase and lipase in the evaluation of acute abdominal pain.Am Surg. 1996 Dec;62(12):1028-33. Am Surg. 1996. PMID: 8955242
-
Management strategy for acute pancreatitis in the JPN Guidelines.J Hepatobiliary Pancreat Surg. 2006;13(1):61-7. doi: 10.1007/s00534-005-1053-5. J Hepatobiliary Pancreat Surg. 2006. PMID: 16463213 Free PMC article.
-
Evaluating tests for acute pancreatitis.Am J Gastroenterol. 1990 Apr;85(4):356-66. Am J Gastroenterol. 1990. PMID: 2183590 Review.
-
Clinical picture and diagnosis of acute pancreatitis.Hepatogastroenterology. 1991 Apr;38(2):97-100. Hepatogastroenterology. 1991. PMID: 1855780 Review.
Cited by
-
Diagnostic Potential of Ratio Between Creatine Kinase and Amylase in Acute Pancreatitis.Mater Sociomed. 2023;35(4):280-284. doi: 10.5455/msm.2023.35.280-284. Mater Sociomed. 2023. PMID: 38380277 Free PMC article.
-
The angle of pancreaticobiliary junction correlates with acute pancreatitis: a magnetic resonance cholangiopancreatography study.Quant Imaging Med Surg. 2015 Jun;5(3):401-6. doi: 10.3978/j.issn.2223-4292.2015.03.13. Quant Imaging Med Surg. 2015. PMID: 26029643 Free PMC article.
-
C-reactive protein/albumin and ferritin as predictive markers for severity and mortality in patients with acute pancreatitis.Prz Gastroenterol. 2023;18(2):168-174. doi: 10.5114/pg.2022.115609. Epub 2022 Apr 20. Prz Gastroenterol. 2023. PMID: 37538281 Free PMC article.
-
Prediction of Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis Using 4-Hour Post-Endoscopic Retrograde Cholangiopancreatography Serum Amylase and Lipase Levels.J Korean Med Sci. 2017 Nov;32(11):1814-1819. doi: 10.3346/jkms.2017.32.11.1814. J Korean Med Sci. 2017. PMID: 28960034 Free PMC article.
-
Comparing the Roles of EUS, ERCP and MRCP in Idiopathic Acute Recurrent Pancreatitis.Clin Med Insights Gastroenterol. 2016 Jun 20;9:35-9. doi: 10.4137/CGast.S37927. eCollection 2016. Clin Med Insights Gastroenterol. 2016. PMID: 27375362 Free PMC article. Review.
References
-
- Malfertheiner P, Kemmer TP. Clinical picture and diagnosis of acute pancreatitis. Hepatogastroenterology. 1991;38:97–100. - PubMed
-
- Corsetti JP, Arvan DA. Acute pancreatitis. In: Black ER, Bordley DR, Tape TG, Panzer RJ, editors. Diagnostic strategies for common medical problems. 2nd ed. Philadelphia: American College of Physicians; 1999. p. 205.
-
- de Dombal F. Acute abdominal pain. An OMGE survey. Scand J Gastroenterol 56 (Suppl) 1979;14:29–43. - PubMed
-
- de Dombal FT. Diagnosis of acute abdominal pain. 2nd ed. London: Churchill Livingstone; 1991. pp. 19–30.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
