

Neurochemical modulation of response inhibition and probabilistic learning in humans
- PMID: 16469930
- PMCID: PMC1867315
- DOI: 10.1126/science.1121218
Neurochemical modulation of response inhibition and probabilistic learning in humans
Abstract
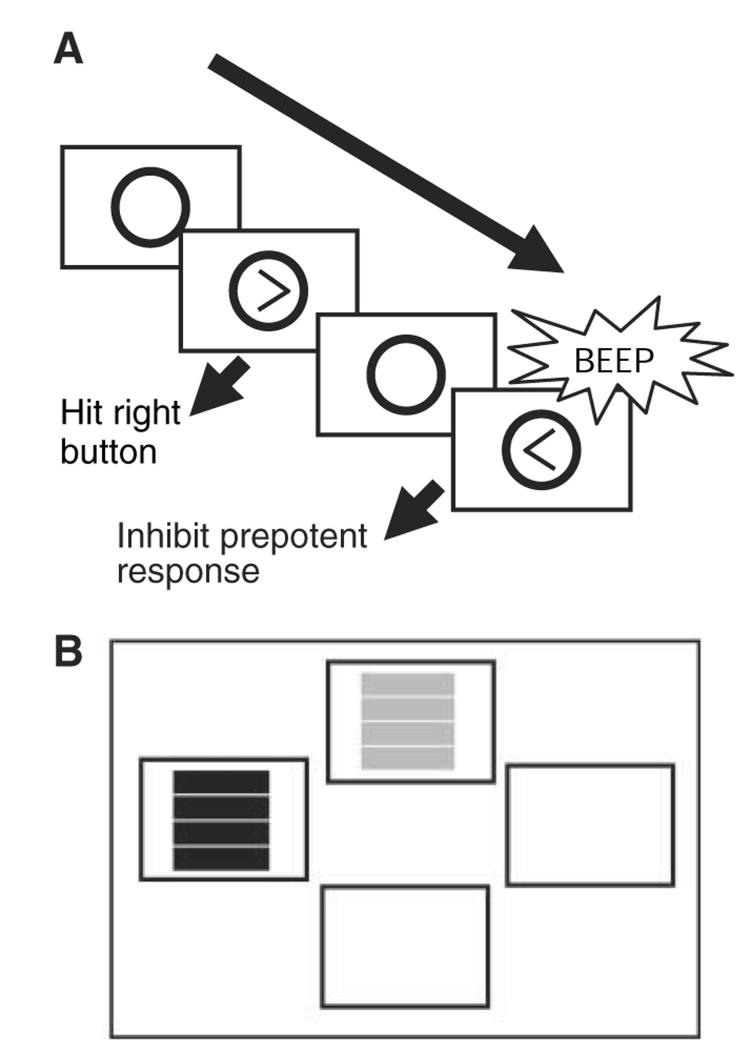
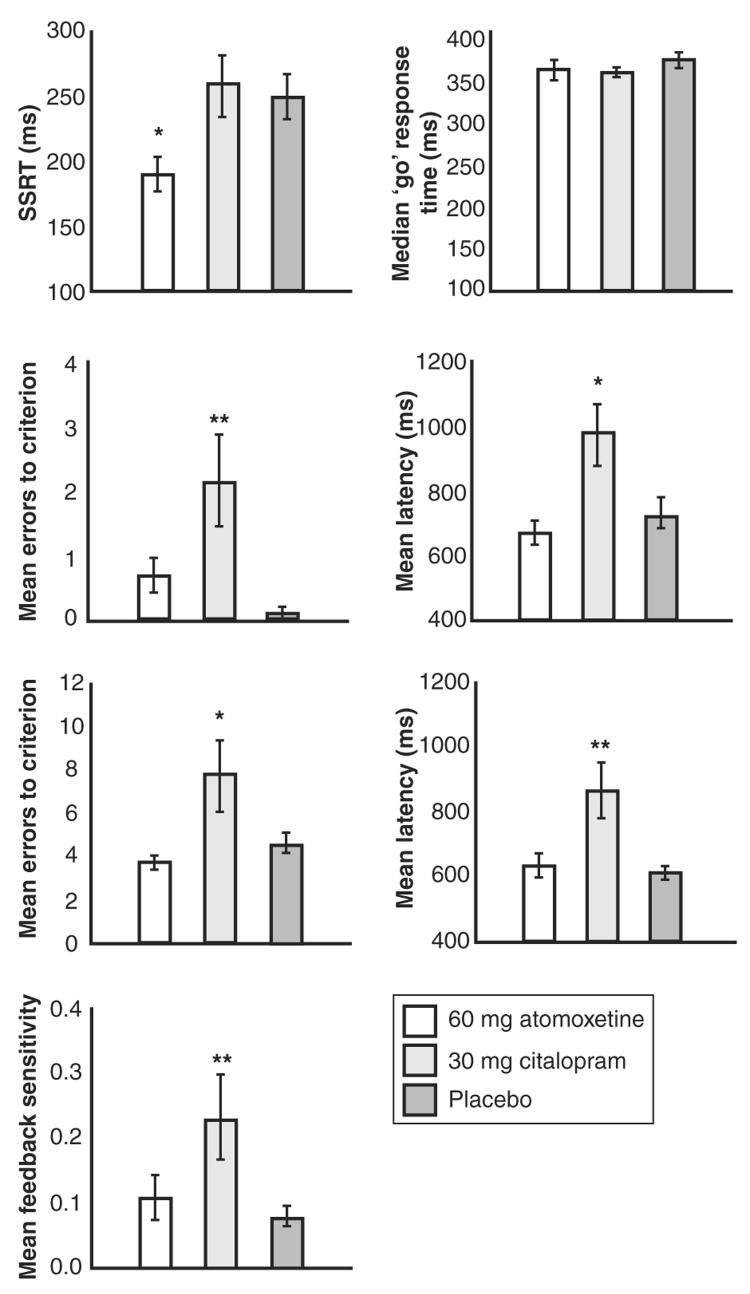
Cognitive functions dependent on the prefrontal cortex, such as the ability to suppress behavior (response inhibition) and to learn from complex feedback (probabilistic learning), play critical roles in activities of daily life. To what extent do different neurochemical systems modulate these two cognitive functions? Here, using stop-signal and probabilistic learning tasks, we show a double dissociation for the involvement of noradrenaline and serotonin in human cognition. In healthy volunteers, inhibition of central noradrenaline reuptake improved response inhibition but had no effect on probabilistic learning, whereas inhibition of central serotonin reuptake impaired probabilistic learning with no effect on response inhibition.
Figures
References
-
- Robbins TW. Prog. Brain Res. 2000;126:469. - PubMed
-
- Chamberlain SR, Sahakian BJ. Curr. Psychiatry Rep. 2004;6:451. - PubMed
-
- Chamberlain SR, Blackwell AD, Fineberg N, Robbins TW, Sahakian BJ. Neurosci. Biobehav. Rev. 2005;29:399. - PubMed
-
- Chamberlain SR, Fineberg NA, Blackwell AD, Robbins TW, Sahakian BJ. Am. J. Psychiatry. in press.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
