

Variability of spinal instrumentation configurations in adolescent idiopathic scoliosis
- PMID: 16477449
- PMCID: PMC2198894
- DOI: 10.1007/s00586-006-0063-6
Variability of spinal instrumentation configurations in adolescent idiopathic scoliosis
Abstract
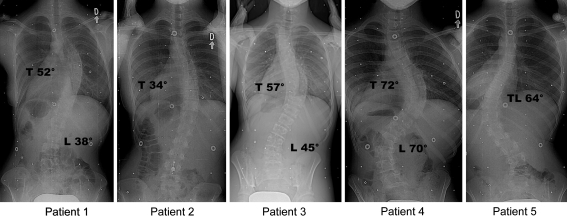
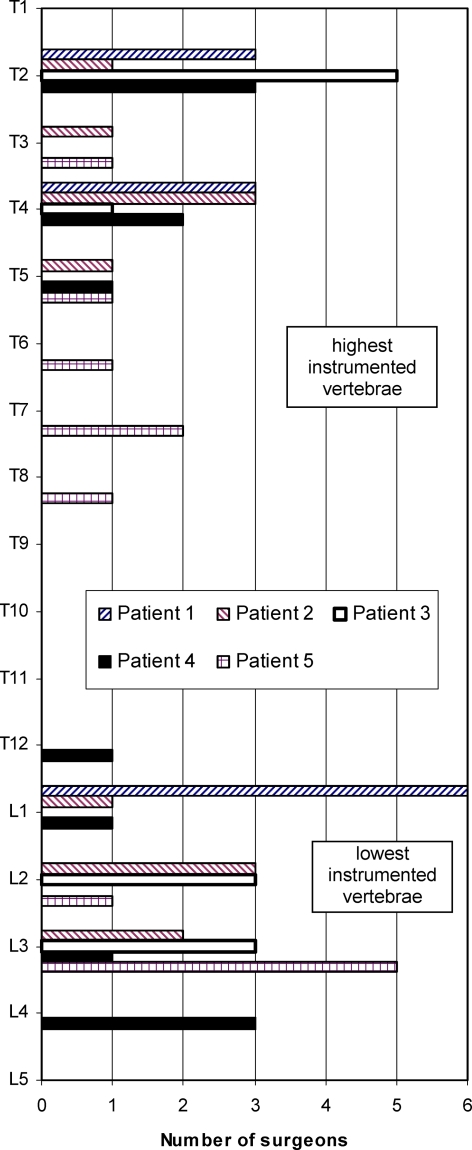
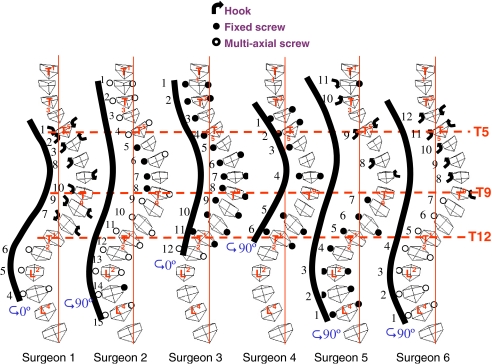
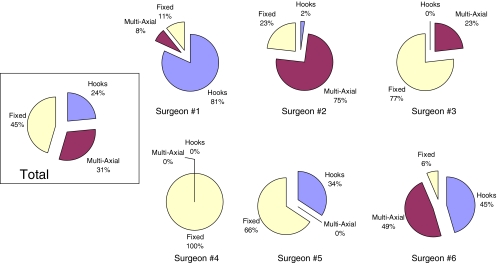
Surgical instrumentation for the correction of adolescent idiopathic scoliosis (AIS) is a complex procedure involving many difficult decisions (i.e. spinal segment to instrument, type/location/number of hooks or screws, rod diameter/length/shape, implant attachment order, amount of rod rotation, etc.). Recent advances in instrumentation technology have brought a large increase in the number of options. Despite numerous clinical publications, there is still no consensus on the optimal surgical plan for each curve type. The objective of this study was to document and analyse instrumentation configuration and strategy variability. Five females (12-19 years) with AIS and an indication for posterior surgical instrumentation and fusion were selected. Curve patterns were as follows: two right thoracic (Cobb: 34 degrees, 52 degrees), two right thoracic and left lumbar (Cobb T/L: 57 degrees/45 degrees, 72 degrees/70 degrees) and 1 left thoraco-lumbar (Cobb: 64 degrees). The pre-operative standing postero-anterior and lateral radiographs, supine side bending radiographs, a three-dimensional (3D) reconstruction of the spine, pertinent 3D measurements as well as clinical information such as age and gender of each patient were submitted to six experienced independent spinal deformity surgeons, who were asked to provide their preferred surgical planning using a posterior spinal approach. The following data were recorded using the graphical user interface of a spine surgery simulator (6x5 cases): implant types, vertebral level, position and 3D orientation of implants, anterior release levels, rod diameter and shape, attachment sequence, rod rotation (angle, direction), adjustments (screw rotation, contraction/distraction), etc. Overall, the number of implants used ranged from 11 to 26 per patient (average 16; SD +/-4). Of these, 45% were mono-axial screws, 31% multi-axial screws and 24% hooks. At one extremity of the spectrum, one surgeon used only mono-axial screws, while at the other, another surgeon used 81% hooks. The selected superior- and inferior-instrumented vertebrae varied up to six and five levels, respectively (STD 1.2 and 1.5). A top-to-bottom attachment sequence was selected in 61% of the cases, a bottom-up in 29% and an alternate order in 11%. The rod rotation maneuver of the first rod varied from 0 degrees (no rotation) to 140 degrees, with a median at 90 degrees. In conclusion, a large variability of instrumentation strategy in AIS was documented within a small experienced group of spinal deformity surgeons. The exact cause of this large variability is unclear but warrants further investigation with multicenter outcome studies as well as experimental and computer simulation studies. We hypothesize that this variability may be attributed to different objectives for correction, to surgeon's personal preferences based on their previous experience, to the known inter-observer variability of current classification systems and to the current lack of clearly defined strategies or rational rules based on the validated biomechanical studies with modern multi-segmental instrumentation systems.
Figures
References
-
- Aubin CE, Descrimes JL, Dansereau J, Skalli W, Lavaste F, Labelle H. Geometrical modeling of the spine and the thorax for the biomechanical analysis of scoliotic deformities using the finite element method (in French) Ann Chir. 1995;49(8):749–761. - PubMed
-
- Bridwell KH. Surgical treatment of adolescent idiopathic scoliosis: the basics and the controversies. Spine. 1994;19:1095–1100. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
