

Diagnostic accuracy of the neurological upper limb examination I: inter-rater reproducibility of selected findings and patterns
- PMID: 16483371
- PMCID: PMC1402320
- DOI: 10.1186/1471-2377-6-8
Diagnostic accuracy of the neurological upper limb examination I: inter-rater reproducibility of selected findings and patterns
Abstract
Background: We have previously assessed the reproducibility of manual testing of the strength in 14 individual upper limb muscles in patients with or without upper limb complaints. This investigation aimed at additionally studying sensory disturbances, the mechanosensitivity of nerve trunks, and the occurrence of physical findings in patterns which may potentially reflect a peripheral neuropathy. The reproducibility of this part of the neurological examination has never been reported.
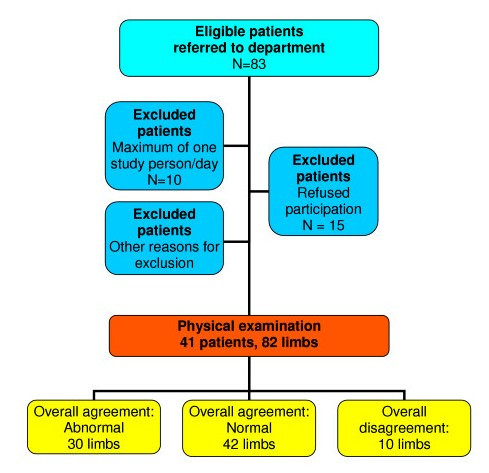
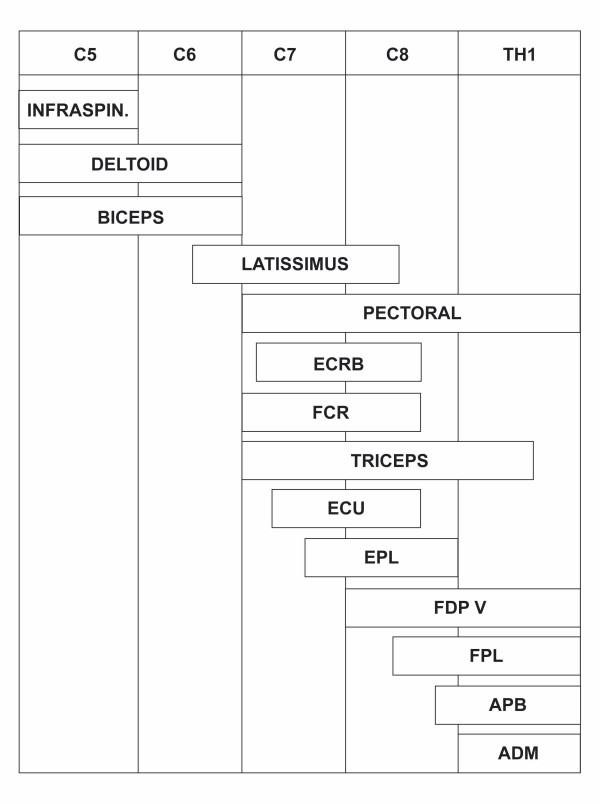
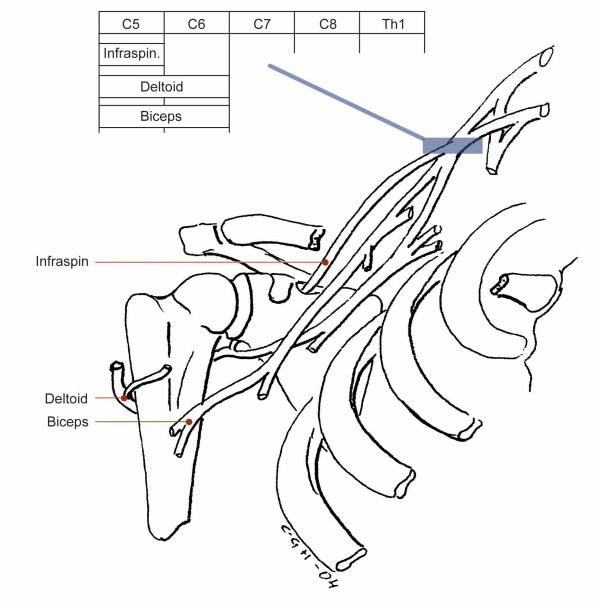
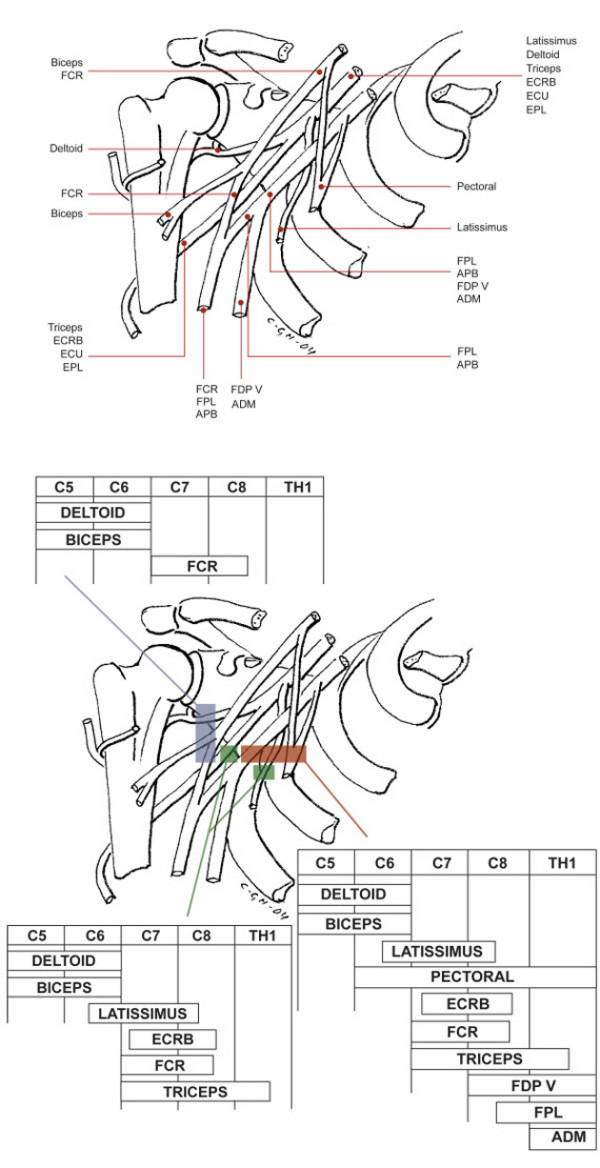
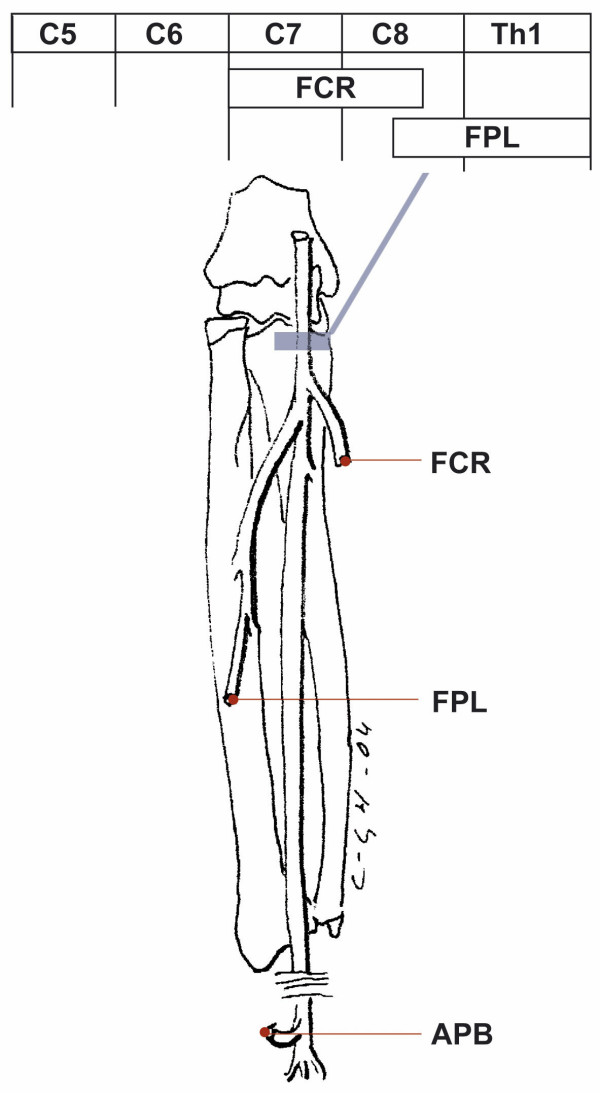
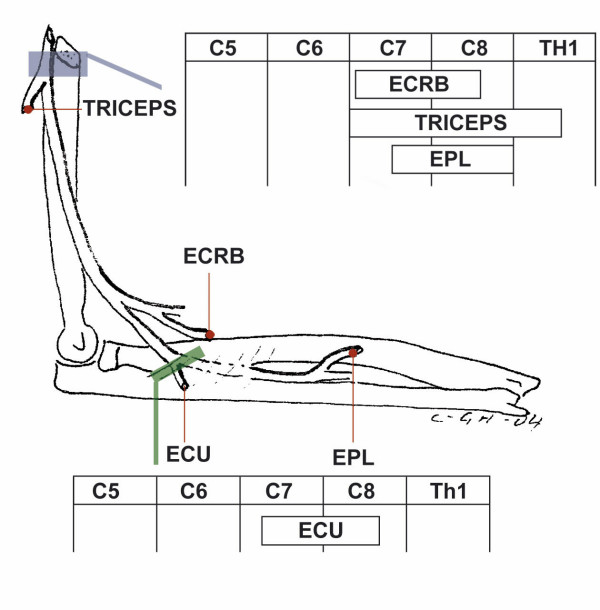
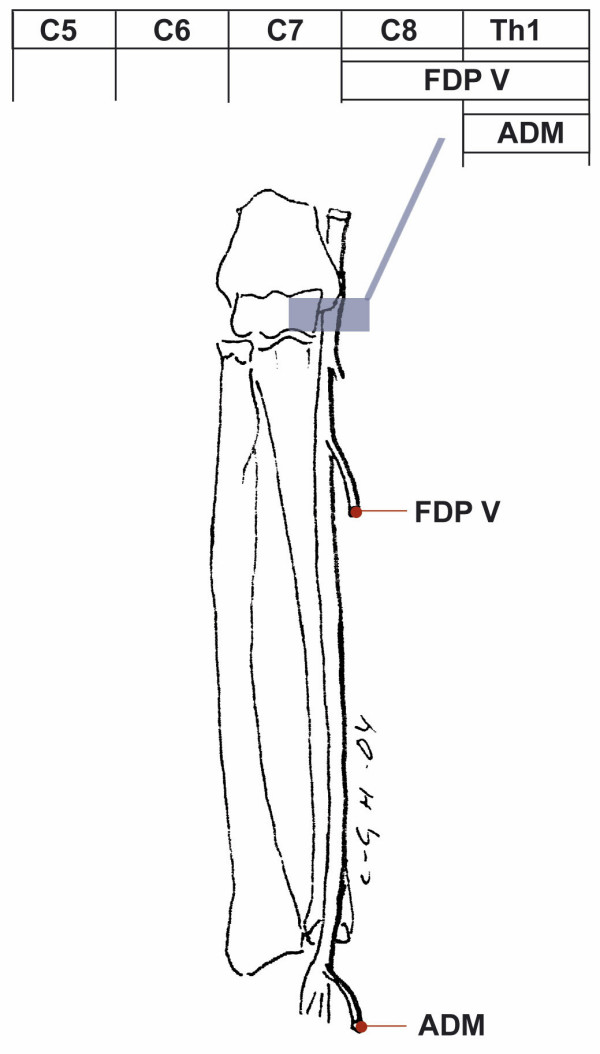
Methods: Two blinded examiners performed a semi-quantitative assessment of 82 upper limbs (strength in 14 individual muscles, sensibility in 7 homonymous territories, and mechanosensitivity of nerves at 10 locations). Based on the topography of nerves and their muscular and cutaneous innervation we defined 10 neurological patterns each suggesting a focal neuropathy. The individual findings and patterns identified by the two examiners were compared.
Results: Strength, sensibility to touch, pain and vibration, and mechanosensitivity were predominantly assessed with moderate to very good reproducibility (median kappa-values 0.54, 0.69, 0.48, 0.58, and 0.53, respectively). The reproducibility of the defined patterns was fair to excellent (median correlation coefficient = 0.75) and the overall identification of limbs with/without pattern(s) was good (kappa = 0.75).
Conclusion: This first part of a study on diagnostic accuracy of a selective neurological examination has demonstrated a promising inter-rater reproducibility of individual neurological items and patterns. Generalization and clinical feasibility require further documentation: 1) Reproducibility in cohorts of other composition, 2) validity with comparison to currently applied standards, and 3) potential benefits that can be attained by the examination.
Figures
References
-
- Quintner J, Elvey R. In: The neurogenic hypothesis of RSI. Bammer G, editor. Canberra, National Centre for Epidemiology and Population Health, The Australian National University; 1991. pp. 1–68. (Working Papers No. 24).
-
- The Nerve Injuries Committee of the Medical Research Council . In: Peripheral nerve injuries. Seddon HJ, editor. London, Her Majesty's Stationary Office; 1954. pp. 1–451. (Medical Research Council Special Report Series No. 282).
-
- Strauch B, Lang A, Ferder M, Keyes-Ford M, Freeman K, Newstein D. The ten test. Plast Reconstr Surg. 1997;99:1074–1078. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
