

Review
doi: 10.1136/bmj.332.7538.407.
Diabetic foot ulcers
Affiliations
- PMID: 16484268
- PMCID: PMC1370976
- DOI: 10.1136/bmj.332.7538.407
Item in Clipboard
Review
Diabetic foot ulcers
BMJ.
.
No abstract available
Figures
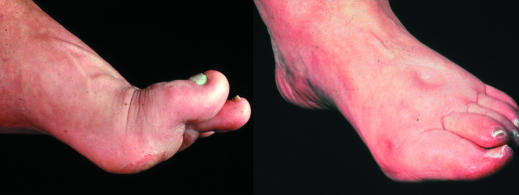
Left: Neuropathic foot with prominent metatarsal heads and pressure points over the plantar forefoot. Right: Neuroischaemic foot showing pitting oedema secondary to cardiac failure, and hallux valgus and erythema from pressure from tight shoe on medial aspect of first metatarsophalangeal joint
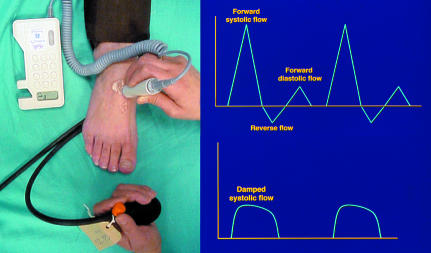
Left: Hand held Doppler used with sphygmomanometer to measure ankle systolic pressure. Right: Doppler waveform from normal foot showing normal triphasic pattern (top) and from neuroischaemic foot showing damped pattern (bottom)

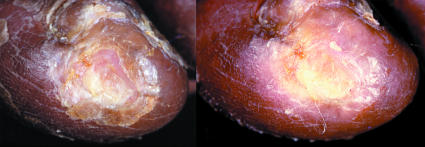
Left: Neuropathic foot with plantar ulcer surrounded by callus. Right: Ulcer over medial aspect of first metatarsophalangeal joint of neuroischaemic foot

Left: Callus removal by sharp debridement. Right: Whitish, macerated, moist tissue under surface of callus, indicating imminent ulceration

Left: Blister under a callus over first metatarsal head. Centre: The roof of the blister is grasped in forceps and cut away, together with associated callus. Right: Ulcer is revealed underneath

Top: Shoe with no proper fastening and with a narrow toe box (left); red marks on toes after wearing unsuitable shoes (right). Left: New ischaemic ulcers resulting from bullae on lateral margin of foot

Top: Shoe with no proper fastening and with a narrow toe box (left); red marks on toes after wearing unsuitable shoes (right). Left: New ischaemic ulcers resulting from bullae on lateral margin of foot
Left: Ischaemic ulcer with halo of thin glassy callus. Right: The halo has been cut away without causing trauma

Left: Vacuum assisted pump sponge attached to plantar aspect of foot. Centre: Pump sponge being removed from foot. Right: Healed wound

Top (left to right): Total contact cast; Aircast prefabricated cast; Scotchcast boot. Left: A suitable shoe bought in the high street may be sufficiently roomy to avoid pressure

Top (left to right): Total contact cast; Aircast prefabricated cast; Scotchcast boot. Left: A suitable shoe bought in the high street may be sufficiently roomy to avoid pressure

Top (left to right): Total contact cast; Aircast prefabricated cast; Scotchcast boot. Left: A suitable shoe bought in the high street may be sufficiently roomy to avoid pressure

Pressure relief ankle/foot orthosis for use with heel ulcers
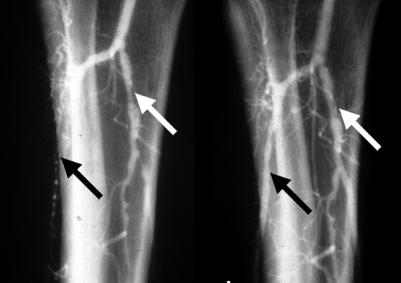
Left: Angiogram showing occlusion of anterior tibial artery and stenosis of tibioperoneal trunk. Right: Post-angioplasty anterior tibial flow has been restored and tibioperoneal stenosis dilated

Left: Necrotic fifth toe and necrotic apices of the first, third, and fourth toes undergoing podiatric debridement. Right: Autoamputation six weeks later, after regular debridement
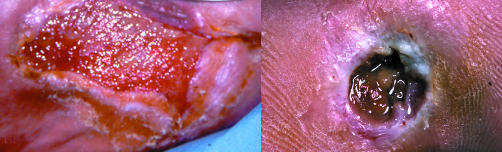
Left: Increased friable granulation tissue. Right: Base of ulcer has areas of yellowish to grey tissue

Left: Deep ulcer with subcutaneous sloughing visible. Centre: Extent of debridement necessary to remove all necrotic tissue down to healthy bleeding tissue. Right: Wound has healed at 10 weeks

Left: Vein bypass seen passing across ankle to the dorsalis pedis artery. Centre: Infected ulcer with cellulitis. Right: Wet necrosis from infected toe ulcer

Left: Vein bypass seen passing across ankle to the dorsalis pedis artery. Centre: Infected ulcer with cellulitis. Right: Wet necrosis from infected toe ulcer

Left: Plantar view of infection after puncture wound that led to wet necrosis of the forefoot requiring amputation of four toes and their adjoining metatarsal heads. Right: Full healing of the large post-surgical tissue defect took six months

Oral hypoglycaemic agent found within the patient's shoe at annual review

Left: Thermal trauma from convection heater. Right: Ulceration after use of foot spa
References
-
- Edmonds M, Foster AVM, Sanders L. A practical manual of diabetic foot care. Oxford: Blackwell Science, 2004.
-
- Bowker JH, Pfeifer MA, eds. Levin and O'Neal's the diabetic foot.6th ed. St Louis: Mosby, 2001.
-
- Boulton AJM, Connor H, Cavanagh PR, eds. The foot in diabetes.3rd ed. Chichester: Wiley, 2000.
-
- The International Working Group on the Diabetic Foot. International consensus on the diabetic foot. 2003 (www.iwgdf.org/concensus/introduction.htm)
-
- Veves A, Giurini JM, Logerfo FW, eds. The diabetic foot. Medical and surgical management. Totowa, NJ: Humana Press, 2002.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical