

Endovascular treatment of posterior cerebral artery aneurysms
- PMID: 16484397
- PMCID: PMC8148799
Endovascular treatment of posterior cerebral artery aneurysms
Abstract
Background and purpose: The purpose of this study was to report the incidence, clinical presentation, endovascular treatment, and outcome of aneurysms of the posterior cerebral artery (PCA).
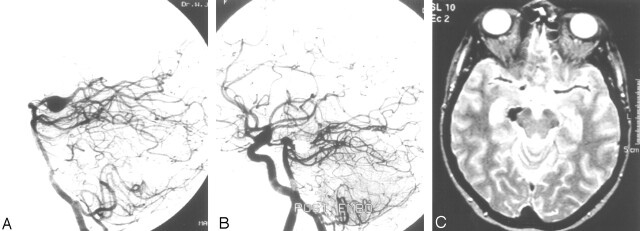
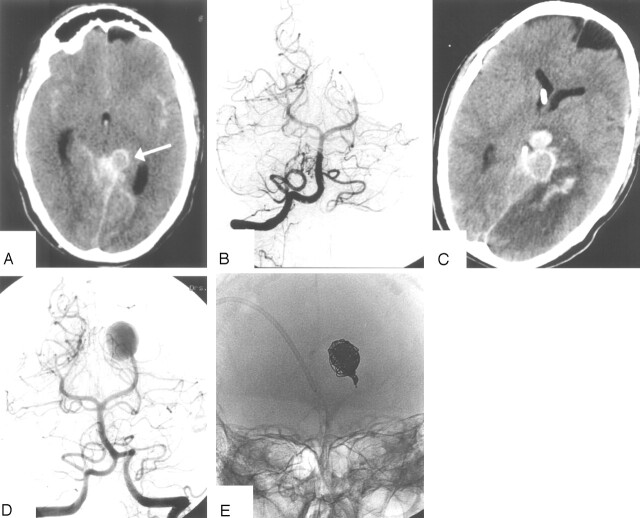
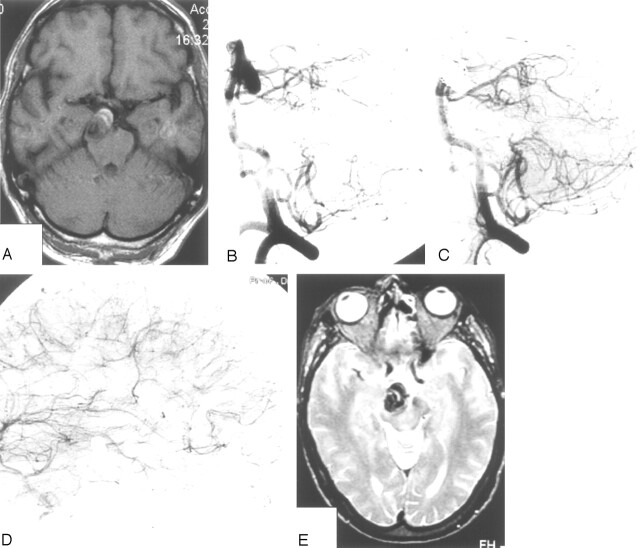
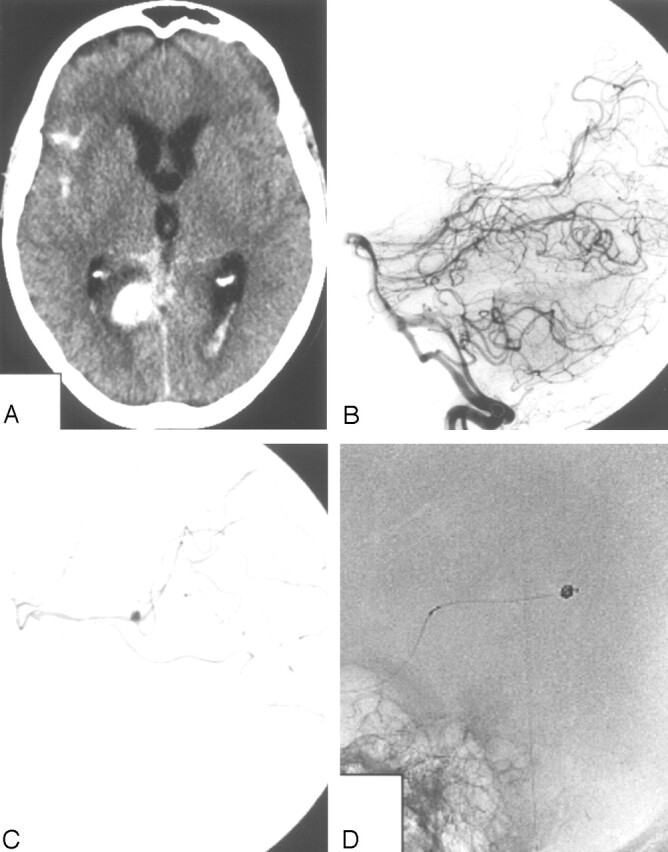
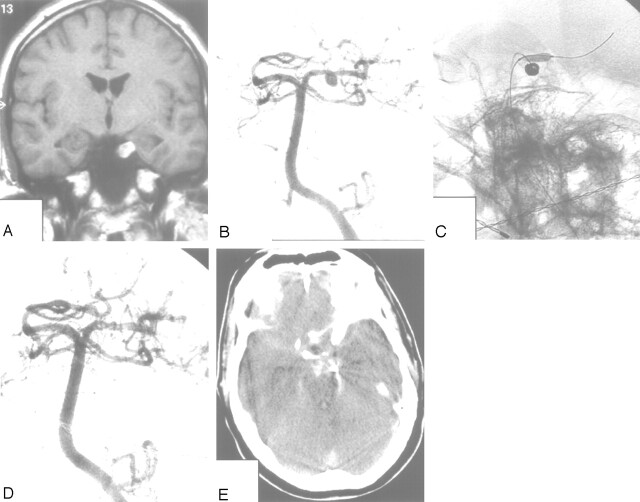
Patients and methods: Among 1880 aneurysms treated between January 1995 and January 2005, 22 aneurysms (1.2%) in 22 patients were located on the PCA. Ten patients presented with subarachnoid hemorrhage (SAH) from the PCA aneurysm: 2 of these patients had additional visual field deficits and 2 had additional occulomotor palsy. One patient presented with acute occulomotor palsy only. Eleven PCA aneurysms were unruptured: 9 were additional to another ruptured aneurysm and 2 were incidentally discovered. Three aneurysms were >15 mm and the other 19 aneurysms were < or = 8 mm. Eighteen aneurysms were saccular, 2 were fusiform, one was dissecting, and one was mycotic.
Results: All aneurysms were successfully treated, 17 with selective occlusion of the aneurysm with coils and 5 with simultaneous occlusion of the aneurysm and parent PCA with coils. There were no complications of treatment. Two patients died of sequelae of SAH shortly after treatment. One patient died 2 months after coiling of an unruptured P1 aneurysm with intramural thrombus of SAH from the same aneurysm. One patient had persistent hemianopsia. In 2 patients with intact visual field in which the parent PCA was occluded, no hemianopsia developed due to sufficient leptomeningeal collateral circulation.
Conclusion: Aneurysms of the PCA are rare with an incidence in our practice of 1.2% of all types of aneurysms. Clinical presentation is variable with SAH, occulomotor palsy, visual field deficit or a combination. Endovascular treatment with either selective occlusion of the aneurysm or occlusion of the aneurysm together with the parent artery with coils is safe and effective with good clinical results.
Figures
References
-
- Drake CG, Peerless SJ, Hernesniemi JA. Surgery of vertebrobasilar aneurysms: London, Ontario experience in 1767 patients. New York: Springer-Verlag;1996. :221–48
-
- Hernesniemi JA, Vapalahti MP, Niskanen M, et al. One-year outcome in early aneurysm surgery: a 14 year experience. Acta Neurochir (Wien) 1993;122:1–10 - PubMed
-
- Peerless SJ, Hernesniemi JA, Gutman FB, et al. Early surgery for ruptured posterior circulation aneurysms. J Neurosurg 1994;80:643–49 - PubMed
-
- Ferrante L, Acqui M, Trillo G, et al. Aneurysms of the posterior cerebral artery: do they present specific characteristics? Acta Neurochir (Wien) 1996;138:840–52 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical