

Comparison of microvascular permeability measurements, K(trans), determined with conventional steady-state T1-weighted and first-pass T2*-weighted MR imaging methods in gliomas and meningiomas
- PMID: 16484420
- PMCID: PMC8148770
Comparison of microvascular permeability measurements, K(trans), determined with conventional steady-state T1-weighted and first-pass T2*-weighted MR imaging methods in gliomas and meningiomas
Abstract
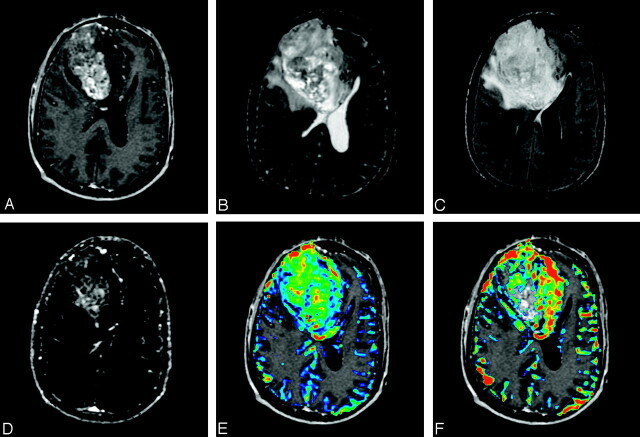
Background and purpose: The widely accepted MR method for quantitating brain tumor microvascular permeability, K(trans), is the steady-state T1-weighted gradient-echo method (ssT1). Recently the first-pass T2*-weighted (fpT2*) method has been used to derive both relative cerebral blood volume (rCBV) and K(trans). We hypothesized that K(trans) derived from the ssT1 and the fpT2* methods will correlate differently in gliomas and meningiomas because of the unique differences in morphologic and functional status of each tumor vascular network.
Methods: Before surgery, 27 patients with newly diagnosed gliomas (WHO grade I-IV; n = 20) or meningiomas (n = 7) underwent conventional anatomic MR imaging and 12 dynamic ssT1 acquisitions followed by 60 dynamic fpT2* images before and after gadopentate dimeglumine administration. The 3 hemodynamic variables-fpT2* rCBV, fpT2* K(trans), and ssT1 K(trans)-were calculated in anatomically identical locations and correlated with glioma grade. The fpT2* K(trans) values were compared with ssT1 K(trans) for gliomas and meningiomas.
Results: All 3 hemodynamic variables displayed distinct distributions among grades 2, 3, and 4 gliomas by using the Kruskal-Wallis test. Only K(trans) values, and not rCBV, could differentiate between grade 4 and lower-grade gliomas by using the Wilcoxon rank sum test. The fpT2* K(trans) was highly predictive of ssT1 K(trans) for gliomas, with an estimated regression coefficient of 0.49 (P < .001). For meningiomas, however, fpT2* K(trans) values correlated poorly with ssT1 K(trans) values (r = 0.26; P = .74).
Conclusion: Compared with rCBV, K(trans) values derived from either ssT1 or fpT2* were more predictive of glioma grade. The fpT2* K(trans) was highly correlated with ssT1 K(trans) in gliomas but not in meningiomas.
Figures





Comment in
-
Permeability versus cerebral blood volume measurement in brain tumor evaluation: comparative clinical value and advice to authors.AJNR Am J Neuroradiol. 2006 Feb;27(2):418-9. AJNR Am J Neuroradiol. 2006. PMID: 16484421 Free PMC article. No abstract available.
References
-
- Provenzale JM, Wang GR, Brenner T, et al. Comparison of permeability in high-grade and low-grade brain tumors using dynamic susceptibility contrast MR imaging. AJR Am J Roentgenol 2002;178:711–16 - PubMed
-
- Stewart PA, Hayakawa K, Farrell CL, et al. Quantitative study of microvessel ultrastructure in human peritumoral brain tissue: evidence for a blood-brain barrier defect. J Neurosurg 1987;67:697–705 - PubMed
-
- Uematsu H, Maeda M, Sadato N, et al. Vascular permeability: quantitative measurement with double-echo dynamic MR imaging: theory and clinical application. Radiology 2000;214:912–17 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical