

Ankle alignment on lateral radiographs. Part 2: reliability and validity of measures
- PMID: 16487459
- PMCID: PMC2267757
- DOI: 10.1177/107110070602700203
Ankle alignment on lateral radiographs. Part 2: reliability and validity of measures
Abstract
Background: In ankles with end-stage osteoarthritis or after total ankle replacement (TAR), radiographic landmarks based on joint surface morphology usually are obscured and inadequate for measurement. Two methods for quantifying anteroposterior tibial-talar alignment without relying on those landmarks were identified in a corollary cadaver-based study. This study aimed to verify reliability and validity of those candidate measures.
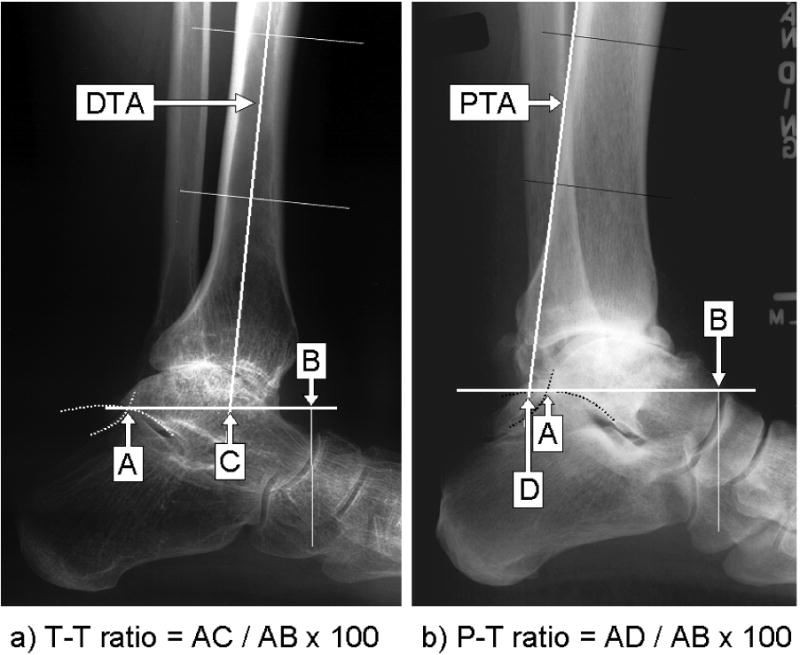
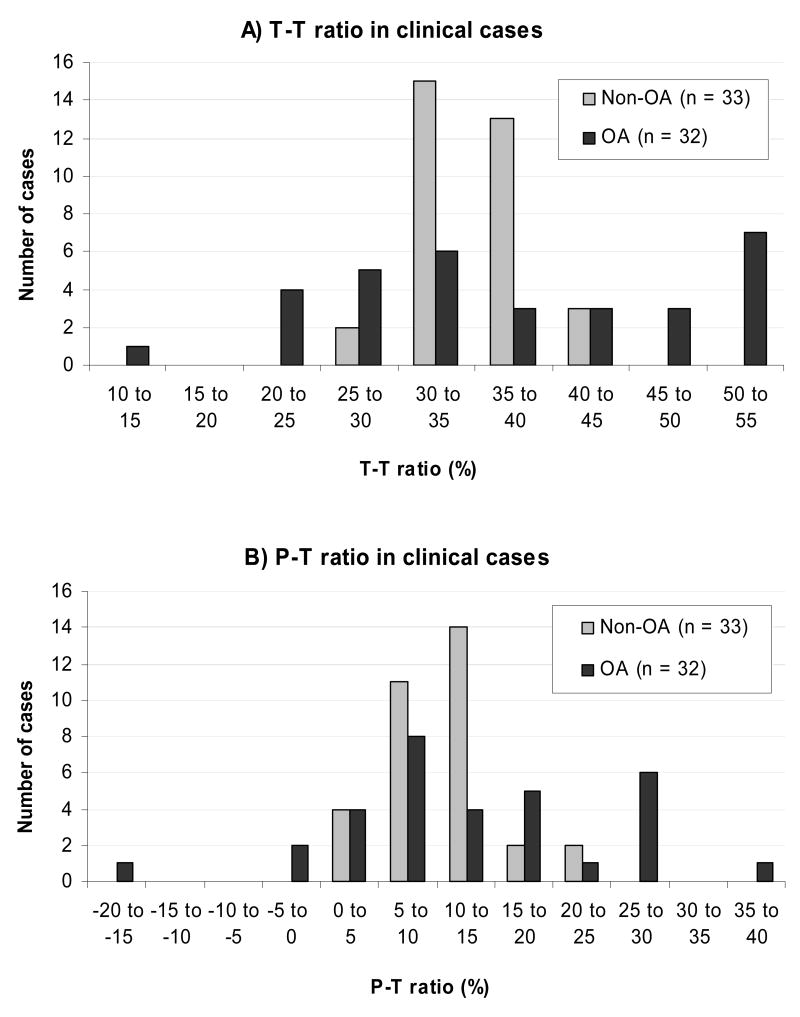
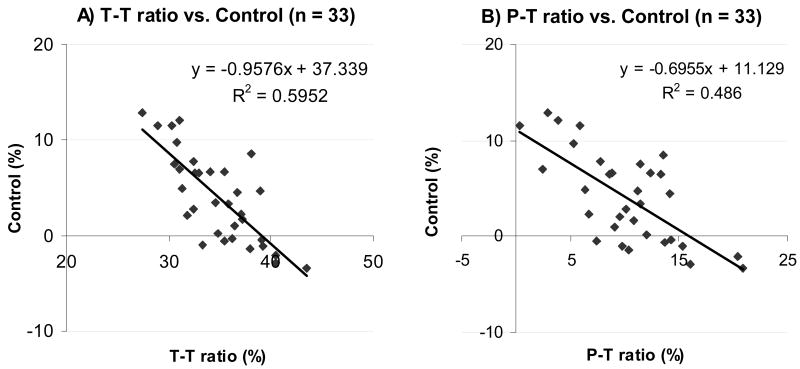
Methods: On clinical radiographs of 33 nonarthritic and 35 arthritic ankles, the anteroposterior tibial-talar alignment was quantified by the two methods; the tibial-axis-to-talus ratio (T-T ratio: the ratio into which the midlongitudinal axis of the tibial shaft divides the longitudinal talar length) and the posterior-tibial-line-to-talus ratio (P-T ratio: a similar ratio, but using the posterior longitudinal line along the tibial shaft). Two observers performed every measurement twice to evaluate intraobserver and interobserver reliability of the candidate measures. For nonarthritic ankles, the anteroposterior tibial-talar alignment was further determined by a control measure that directly quantified orientation of the talar dome relative to the tibial shaft. Correlation of the T-T and P-T ratios with the control measure was then evaluated for validity.
Results: Measurement of the T-T ratio with arthritic ankles was highly reproducible with the coefficients of determination (R(2)) greater than 0.95, for either interobserver or intraobserver. Correlation between this measure and the control measure was supported (R(2) = 0.60, p < 0.0001). Reliability of the P-T ratio also was strong (R(2) > 0.91), although both reliability and validity of this measure were relatively inferior to the T-T ratio.
Conclusions: The T-T ratio reliably and validly described the anteroposterior tibial-talar alignment on clinical radiographs, regardless of the condition of ankle joint surface. This measure appears to be a reliable radiographic measure for determining the magnitude of anteroposterior talar subluxation in ankles with articular degeneration or after TAR and can facilitate clinical investigations.
Figures
References
-
- Conti SF, Wong YS. Complications of total ankle replacement. Clin Orthop. 2001;391:105–114. - PubMed
-
- Myerson MS, Mroczek K. Perioperative complications of total ankle arthroplasty. Foot Ankle Int. 2003;24:17–21. - PubMed
-
- Pyevich MT, Saltzman CL, Callaghan JJ, Alvine FG. Total ankle arthroplasty: A unique design. J Bone Joint Surg. 1998;80-A:1410–1420. - PubMed
-
- Saltzman CL, Tochigi Y, Rudert MJ, McIff TE, Brown TD. The effect of Agility ankle prosthesis misalignment on the peri-ankle ligaments. Clin Orthop. 2004;424:137–42. - PubMed
-
- Takakura Y, Tanaka Y, Kumai T, Tamai S. Low tibial osteotomy for osteoarthritis of the ankle; results of a new operation in 18 patients. J Bone Joint Surg. 1995;77-B:50–54. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
