

Favorable outcomes of hilar duct oriented hepatic resection for high grade Tsunoda type hepatolithiasis
- PMID: 16489644
- PMCID: PMC4066063
- DOI: 10.3748/wjg.v12.i3.431
Favorable outcomes of hilar duct oriented hepatic resection for high grade Tsunoda type hepatolithiasis
Abstract
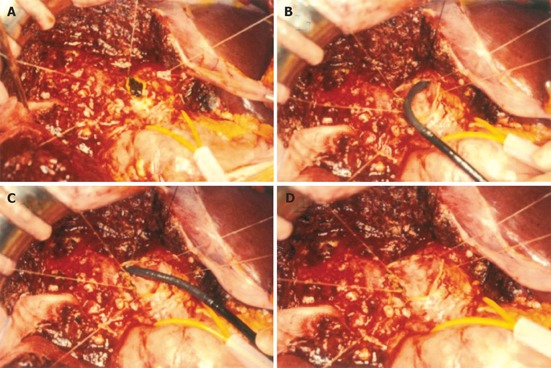
Aim: To evaluate the efficacy of hilar duct oriented hepatectomy for intractable hepatolithiasis, the ventral hilum exposure (VHE) method that has been applied by the authors.
Methods: From June 1994 to June 2004 for a period of 10 years, 153 patients who had Tsunoda type III or IV hepatolithiasis, received hepatectomy at our institution. Among these patients, 128 who underwent hepatectomy by the VHE method were the subjects for the study. We analyzed the risk of this procedure, residual rate of intra-hepatic stones, and stone recurrent rates.
Results: The average age was 54.2 years, and the male to female ratio was 1:1.7. The average follow-up period was 25.6 mo (6-114 mo). There was no post-operative severe complication or mortality after the operation. The rate of residual stones was 5.4% and the rate of recurrent stones was 4.2%.
Conclusion: VHE is a safe surgical procedure and provides favorable treatment results of intractable hepatolithiasis. Especially, this procedure has advantage in that intra-hepatic bile duct stricture may be confirmed and corrected directly during surgery.
Figures



References
-
- Chen MF, Jan YY, Wang CS, Hwang TL, Jeng LB, Chen SC, Chen TJ. A reappraisal of cholangiocarcinoma in patient with hepatolithiasis. Cancer. 1993;71:2461–2465. - PubMed
-
- Kubo S, Kinoshita H, Hirohashi K, Hamba H. Hepatolithiasis associated with cholangiocarcinoma. World J Surg. 1995;19:637–641. - PubMed
-
- Park YH, Park SJ, Jang JY, Ahn YJ, Park YC, Yoon YB, Kim SW. Changing patterns of gallstone disease in Korea. World J Surg. 2004;28:206–210. - PubMed
-
- Cetta F, Lombardo F, Cariati A. The role of the content (decreased level of apolipoprotein A1) and of the container (bile duct stricture, sectorial dilatation of the ducts determining bile stasis) in the pathogenesis of hepatolithiasis, either pigment or cholesterol. Hepatology. 1994;19:1539–1541. - PubMed
-
- Nakanuma Y, Yamaguchi K, Ohta G, Terada T. Pathologic features of hepatolithiasis in Japan. Hum Pathol. 1988;19:1181–1186. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
