

Long-term outcomes of hepatectomy vs percutaneous ablation for treatment of hepatocellular carcinoma < or =4 cm
- PMID: 16489666
- PMCID: PMC4066085
- DOI: 10.3748/wjg.v12.i4.546
Long-term outcomes of hepatectomy vs percutaneous ablation for treatment of hepatocellular carcinoma < or =4 cm
Abstract
Aim: To determine which treatment modality--hepatectomy or percutaneous ablation--is more beneficial for patients with small hepatocellular carcinoma (HCC) (< or =4 cm) in terms of long-term outcomes.
Methods: A retrospective analysis of 149 patients with HCC < or =4 cm was conducted. Eighty-five patients underwent partial hepatectomy (anatomic in 47 and non-anatomic in 38) and 64 underwent percutaneous ablation (percutaneous ethanol injection in 37, radiofrequency ablation in 21, and microwave coagulation in 6). The median follow-up period was 69 mo.
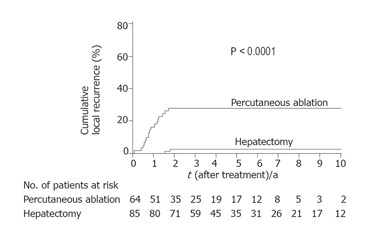
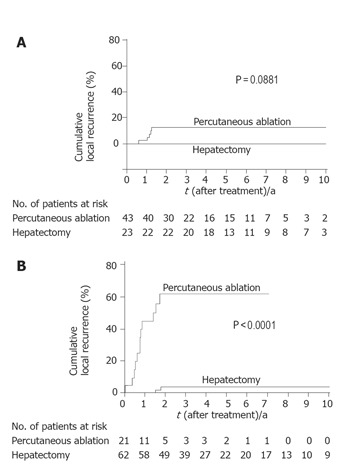
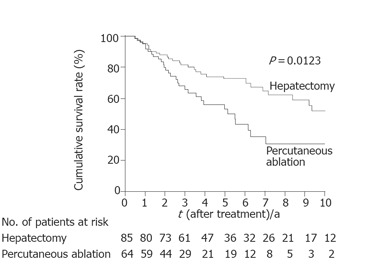
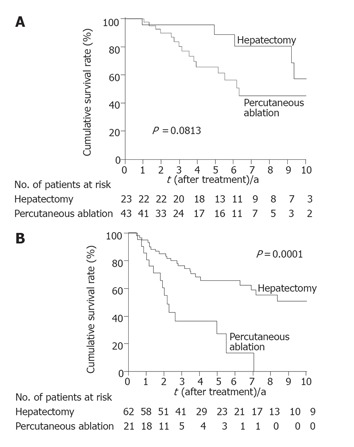
Results: Hepatectomy was associated with larger tumor size (P<0.001), whereas percutaneous ablation was significantly associated with impaired hepatic functional reserve. Local recurrence was less frequent following hepatectomy (P<0.0001). Survival was better following hepatectomy (median survival time: 122 mo) than following percutaneous ablation (median survival time: 66 mo; P=0.0123). When tumor size was divided into < or =2 cm vs >2 cm, the favorable effects of hepatectomy on long-term survival was seen only in patients with tumors>2 cm (P=0.0001). The Cox proportional hazards regression model revealed that hepatectomy (P=0.006) and tumors < or =2 cm (P=0.017) were independently associated with better survival.
Conclusion: Hepatectomy provides both better local control and better long-term survival for patients with HCC < or =4 cm compared with percutaneous ablation. Of the patients with HCC < or =4 cm, those with tumors >2 cm are good candidates for hepatectomy, provided that the hepatic functional reserve of the patient permits resection.
Figures
References
-
- Bruix J, Llovet JM. Prognostic prediction and treatment strategy in hepatocellular carcinoma. Hepatology. 2002;35:519–524. - PubMed
-
- Imamura H, Matsuyama Y, Miyagawa Y, Ishida K, Shimada R, Miyagawa S, Makuuchi M, Kawasaki S. Prognostic significance of anatomical resection and des-gamma-carboxy prothrombin in patients with hepatocellular carcinoma. Br J Surg. 1999;86:1032–1038. - PubMed
-
- Montorsi M, Santambrogio R, Bianchi P, Donadon M, Moroni E, Spinelli A, Costa M. Survival and recurrences after hepatic resection or radiofrequency for hepatocellular carcinoma in cirrhotic patients: a multivariate analysis. J Gastrointest Surg. 2005;9:62–7; discussion 67-8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
