

Distal small bowel motility and lipid absorption in patients following abdominal aortic aneurysm repair surgery
- PMID: 16489672
- PMCID: PMC4066091
- DOI: 10.3748/wjg.v12.i4.582
Distal small bowel motility and lipid absorption in patients following abdominal aortic aneurysm repair surgery
Abstract
Aim: To investigate distal small bowel motility and lipid absorption in patients following elective abdominal aortic aneurysm (AAA) repair surgery.
Methods: Nine patients (aged 35-78 years; body mass index (BMI) range: 23-36 kg/m(2)) post-surgery for AAA repair, and seven healthy control subjects (20-50 years; BMI range: 21-29 kg/m(2)) were studied. Continuous distal small bowel manometry was performed for up to 72 h, during periods of fasting and enteral feeding (Nutrison). Recordings were analyzed for the frequency, origin, length of migration, and direction of small intestinal burst activity. Lipid absorption was assessed on the first day and the third day post surgery in a subset of patients using the (13)C-triolein-breath test, and compared with healthy controls. Subjects received a 20-min intraduodenal infusion of 50 mL liquid feed mixed with 200 microL (13)C-triolein. End-expiratory breath samples were collected for 6 h and analyzed for (13)CO(2) concentration.
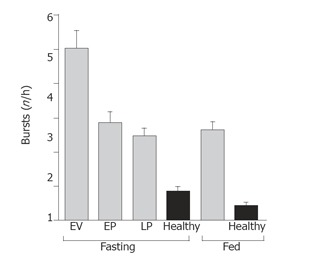
Results: The frequency of burst activity in the proximal and distal small intestine was higher in patients than in healthy subjects, under both fasting and fed conditions (P<0.005). In patients there was a higher proportion of abnormally propagated bursts (71% abnormal), which began to normalize by d 3 (25% abnormal) post-surgery. Lipid absorption data was available for seven patients on d 1 and four patients on d 3 post surgery. In patients, absorption on d 1 post-surgery was half that of healthy control subjects (AUC (13)CO(2) 1323+/-244 vs 2646+/-365; P<0.05, respectively), and was reduced to the one-fifth that of healthy controls by d 3 (AUC (13)CO(2) 470+/-832 vs 2646+/-365; P<0.05, respectively).
Conclusion: Both proximal and distal small intestinal motor activity are transiently disrupted in critically ill patients immediately after major surgery, with abnormal motility patterns extending as far as the ileum. These motor disturbances may contribute to impaired absorption of enteral nutrition, especially when intraluminal processing is necessary for efficient digestion.
Figures




References
-
- Heyland D, Cook DJ, Winder B, Brylowski L, Van deMark H, Guyatt G. Enteral nutrition in the critically ill patient: a prospective survey. Crit Care Med. 1995;23:1055–1060. - PubMed
-
- Montejo JC. Enteral nutrition-related gastrointestinal complications in critically ill patients: a multicenter study. The Nutritional and Metabolic Working Group of the Spanish Society of Intensive Care Medicine and Coronary Units. Crit Care Med. 1999;27:1447–1453. - PubMed
-
- Ritz MA, Fraser R, Edwards N, Di Matteo AC, Chapman M, Butler R, Cmielewski P, Tournadre JP, Davidson G, Dent J. Delayed gastric emptying in ventilated critically ill patients: measurement by 13 C-octanoic acid breath test. Crit Care Med. 2001;29:1744–1749. - PubMed
-
- Montejo JC, Grau T, Acosta J, Ruiz-Santana S, Planas M, García-De-Lorenzo A, Mesejo A, Cervera M, Sánchez-Alvarez C, Núñez-Ruiz R, et al. Multicenter, prospective, randomized, single-blind study comparing the efficacy and gastrointestinal complications of early jejunal feeding with early gastric feeding in critically ill patients. Crit Care Med. 2002;30:796–800. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
