

Expression and possible prognostic role of MAGE-A4, NY-ESO-1, and HER-2 antigens in women with relapsing invasive ductal breast cancer: retrospective immunohistochemical study
- PMID: 16489695
- PMCID: PMC2080373
Expression and possible prognostic role of MAGE-A4, NY-ESO-1, and HER-2 antigens in women with relapsing invasive ductal breast cancer: retrospective immunohistochemical study
Abstract
Aim: To evaluate the possible prognostic role of the expression of MAGE-A4 and NY-ESO-1 cancer/testis antigens in women diagnosed with invasive ductal breast cancer and determine the expression of HER-2 antigen.
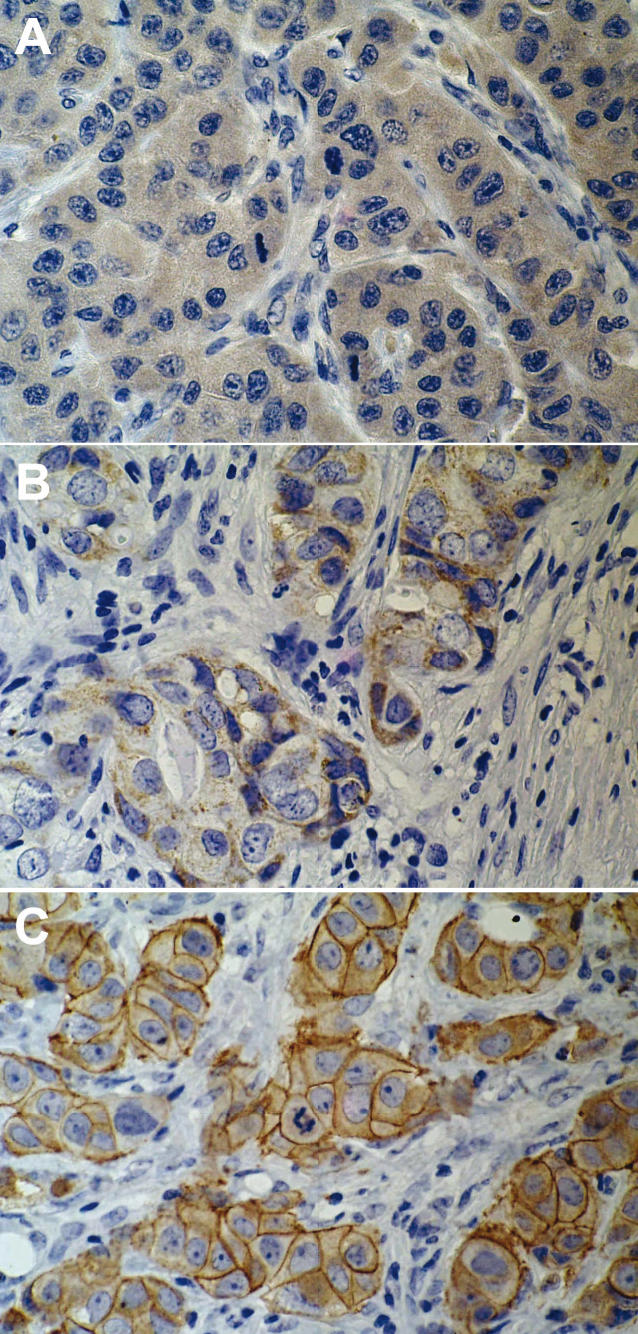
Methods: The expression of MAGE-A4, NY-ESO-1, and HER-2 antigens was evaluated immunohistochemically on archival paraffin-embedded samples of breast cancer tissue from 81 patients. All patients had T1 to T3, N0 to N1, M0 tumors and underwent postoperative radiotherapy and, if indicated, systemic therapy (chemotherapy and hormonal therapy). The antigen expression in women who were disease-free for 5 years of follow up (n=23) was compared with that in women with either locoregional relapse (n=30) or bone metastases (n=28). Patient survival after 10 years of follow up was assessed.
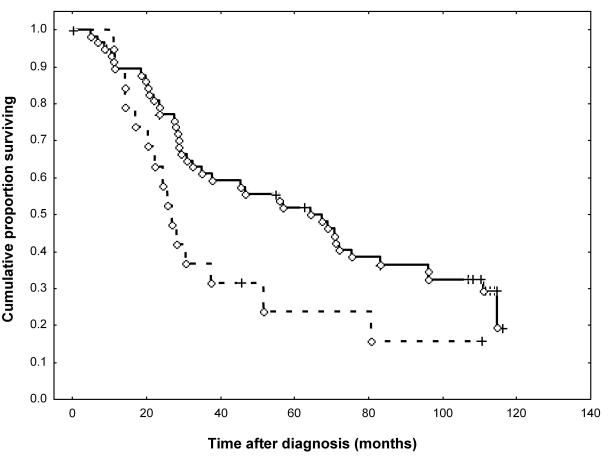
Results: The three groups of women were comparable in terms of age, type of operation, tumor size, tumor grade, number of metastatically involved axillary lymph nodes, Nottingham prognostic index (NPI), progesterone receptor (PR) status, and adjuvant hormonal therapy. Estrogen receptors (ER) were positive in 13 women in the 5-year relapse-free group vs 8 in locoregional relapse and 7 in bone metastases group (P=0.032). There were significantly fewer women who received adjuvant chemotherapy in the 5-year relapse-free group than in other two groups (7 vs 23 with locoregional relapse and 25 with bone metastases; P<0.001). This group also had a significantly better 10-year survival (14 women vs 1 with locoregional relapse and 1 with bone metastases; P<0.001). The three groups did not differ in the NY-ESO-1 or HER-2 expression, but the number of patients expressing MAGE-A4 antigen was significantly lower in the group with locoregional relapse (P=0.014). In all groups, MAGE-A4 antigen expression was associated with the NY-ESO-1 antigen expression (P=0.006), but not with tumor size and grade, number of metastatically involved axillary lymph nodes, or the ER and PR status. MAGE-A4-positive patients had a significantly longer survival than the MAGE-A4-negative patients (P=0.046). This was not observed with NY-ESO-1 and HER-2 antigens.
Conclusion: Our results suggest that the MAGE-A4 antigen may be used as a tumor marker of potential prognostic relevance.
Figures
References
-
- Chang JC, Hilsenbeck SG. Prognostic and predictive markers. In: Harris JR, Lippman ME, Morrow M, Osborne CK, editors. Diseases of the breast. 3rd ed. Philadelphia (PA): Lippincott, Williams and Wilkins; 2004. p. 675-96.
-
- Goldhirsch A, Glick JH, Gelber RD, Coates AS, Thurlimann B, Senn HJ. Meeting highlights: international expert consensus on the primary therapy of early breast cancer. Ann Oncol. 2005;16:1569–83. - PubMed
-
- Colozza M, Cardoso F, Sotiriou C, Larsimont D, Piccart MJ. Bringing molecular prognosis and prediction to the clinic. Clin Breast Cancer. 2005;6:61–76. - PubMed
-
- Keen JC, Davidson NE. The biology of breast carcinoma. Cancer. 2003;97(suppl 3):825–33. - PubMed
-
- Cianfrocca M, Goldstein LJ. Prognostic and predictive factors in early-stage breast cancer. Oncologist. 2004;9:606–16. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous