

Telomerase peptide vaccination: a phase I/II study in patients with non-small cell lung cancer
- PMID: 16491401
- PMCID: PMC11030882
- DOI: 10.1007/s00262-006-0145-7
Telomerase peptide vaccination: a phase I/II study in patients with non-small cell lung cancer
Abstract
Purpose: A phase I/II study was conducted to investigate the safety, tolerability and clinical response to vaccination with a combination of telomerase peptides GV1001 (hTERT: 611-626) and HR2822 (hTERT: 540-548) in patients with non-small cell lung cancer.
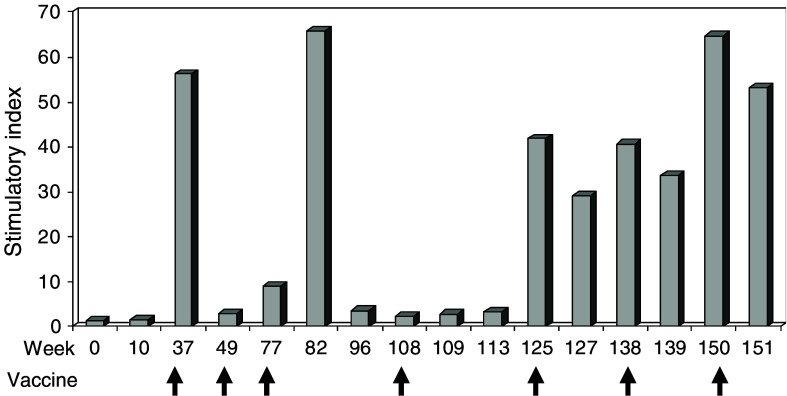
Experimental design: Twenty-six patients with non-small cell lung cancer received intradermal administrations of either 60 nmole (112 microg) or 300 nmole (560 microg) GV1001 in combination with 60 nM (68.4 microg) HR2822 and granulocyte macrophage-colony stimulating factor. The treatment period was 10 weeks. Booster vaccinations with 300 nM GV1001 were offered as follow-up. Monitoring of blood samples, clinical examination and radiological staging were performed regularly. Immune responses were measured as delayed-type hypersensitivity skin reaction and in vitro T cell proliferation. Bone marrow function was monitored in long time survivors.
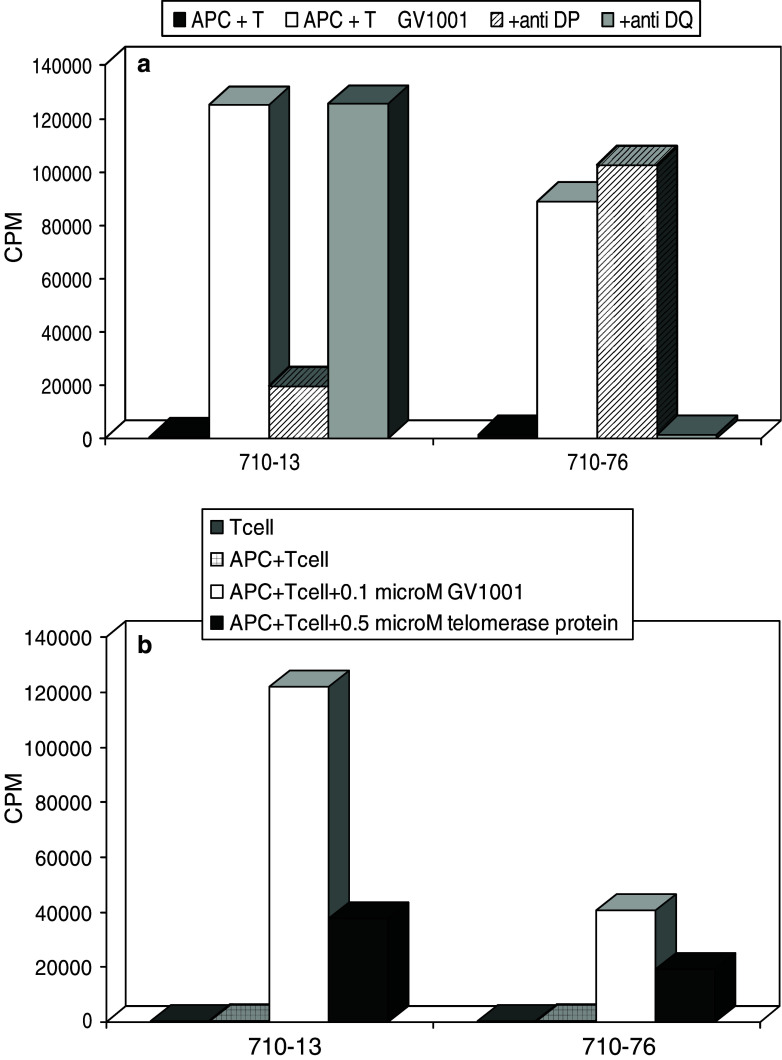
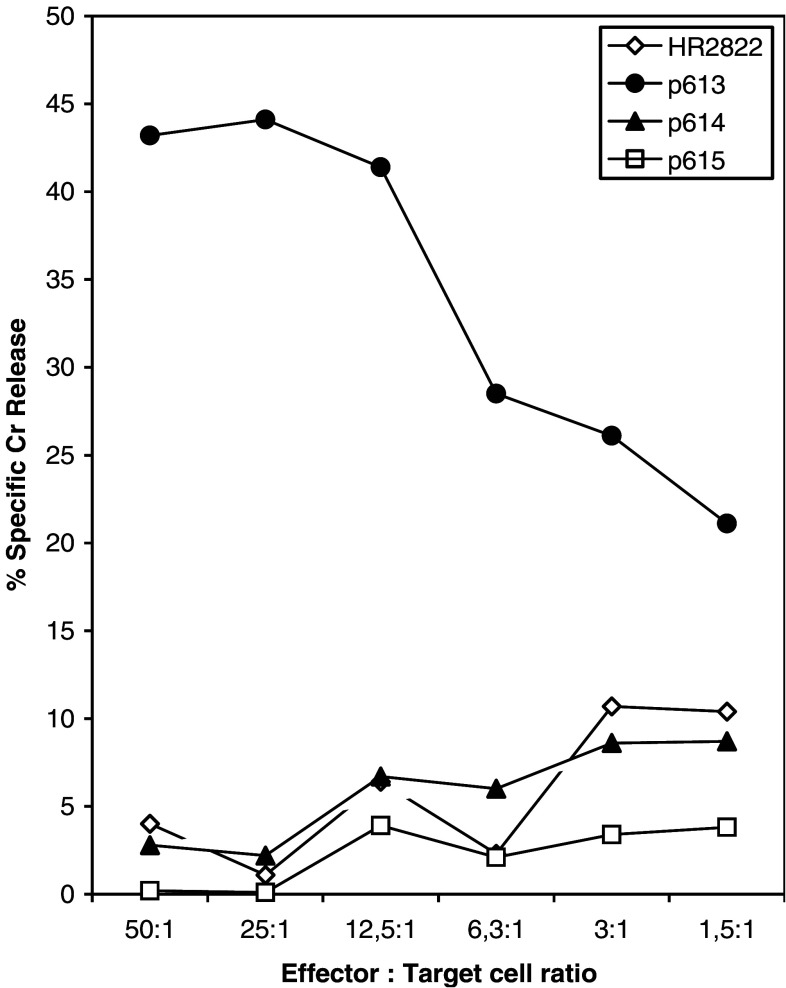
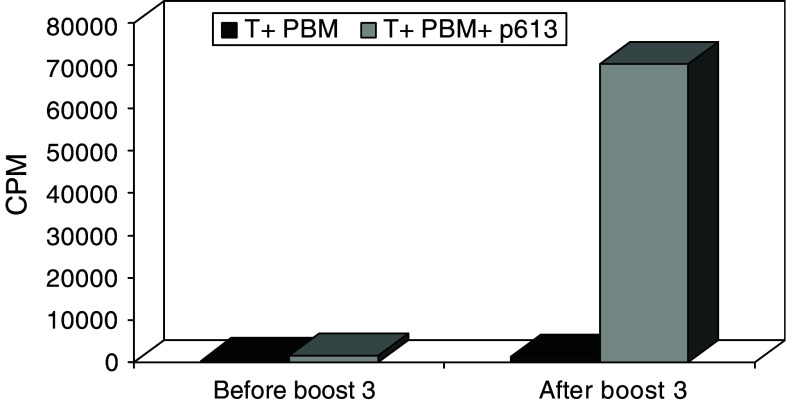
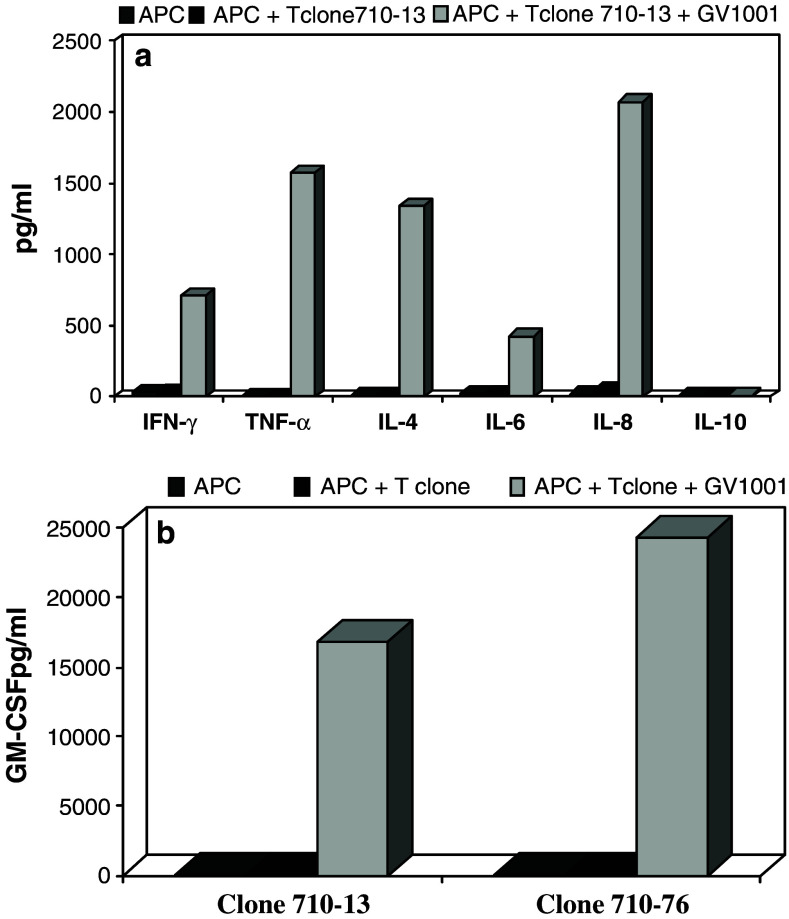
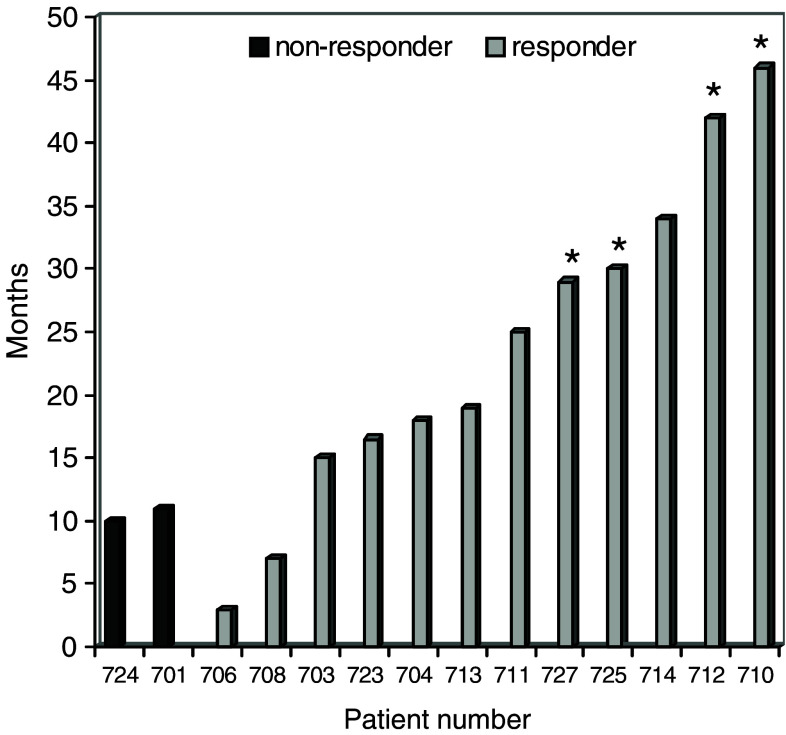
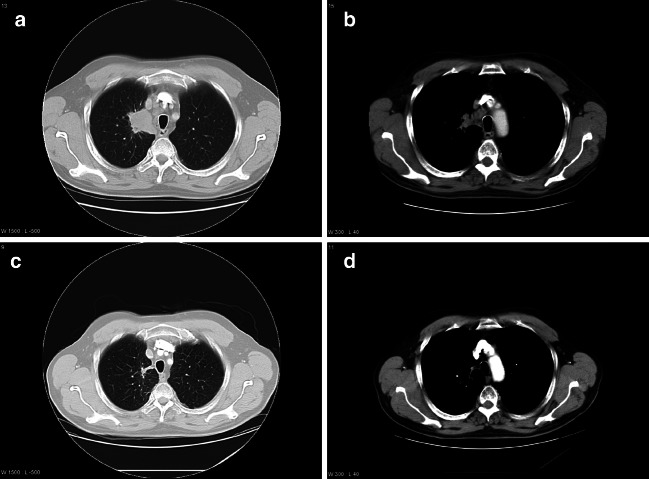
Results: The treatment was well tolerated with minor side effects. No bone marrow toxicities were observed in long time survivors with immune responses. Immune responses against GV1001 were detected in 11 of 24 evaluable patients during the primary regimen and in additional two patients following booster injections. Two patients responded to HR2822. Cloned GV1001-specific CD4+ T cells displayed a Th1 cytokine profile and recognized autologous antigen presenting cells pulsed with recombinant telomerase protein. A complete tumor response was observed in one patient who developed GV1001-specific cytotoxic T cells that could be cloned from peripheral blood.
Conclusion: The results demonstrate that GV1001 and HR2822 are immunogenic and safe to use in patients with NSCLC. Induction of GV1001-specific immune responses may result in objective tumor responses. Based on these initial encouraging results, further clinical studies of GV1001 in NSCLC patients are warranted.
Figures
References
-
- Shepherd F, Carney D (2000) In: Hansen H (ed) Treatment of NSCLC in Textbook of lung cancer. Martin Dunitz
-
- Woo Ey, Yeh H, Chu S, et al. Cutting edge; regulatory T cells from lung cancer patients directly inhibit autologous T cell proliferation. J Immunol. 2002;168:4272–4276. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
