

Laparoscopic sphincter-preserving total mesorectal excision with colonic J-pouch reconstruction: five-year results
- PMID: 16495700
- PMCID: PMC1448945
- DOI: 10.1097/01.sla.0000202180.16723.03
Laparoscopic sphincter-preserving total mesorectal excision with colonic J-pouch reconstruction: five-year results
Abstract
Objective: To prospectively evaluate the oncologic and functional outcomes of laparoscopic total mesorectal excision (TME) with colonic J-pouch reconstruction.
Background: TME is considered the established gold standard in rectal cancer surgery. However, data on laparoscopic sphincter-preserving TME are limited.
Methods: Patients with mid or low rectal cancer underwent laparoscopic TME with colonic J-pouch reconstruction by a single surgical team. Clinical and oncologic data were prospectively recorded and analyzed.
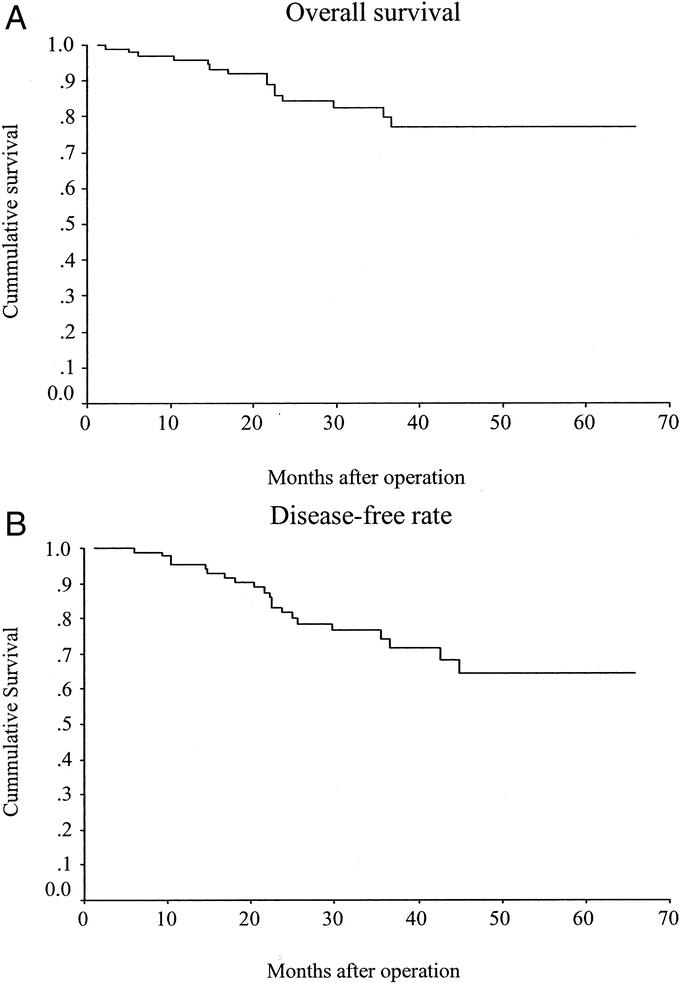
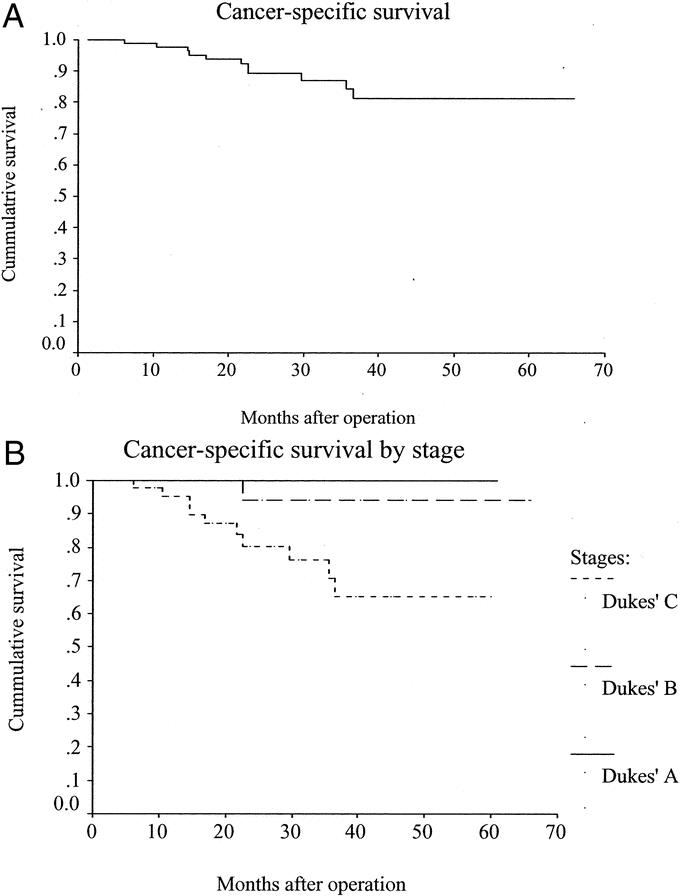
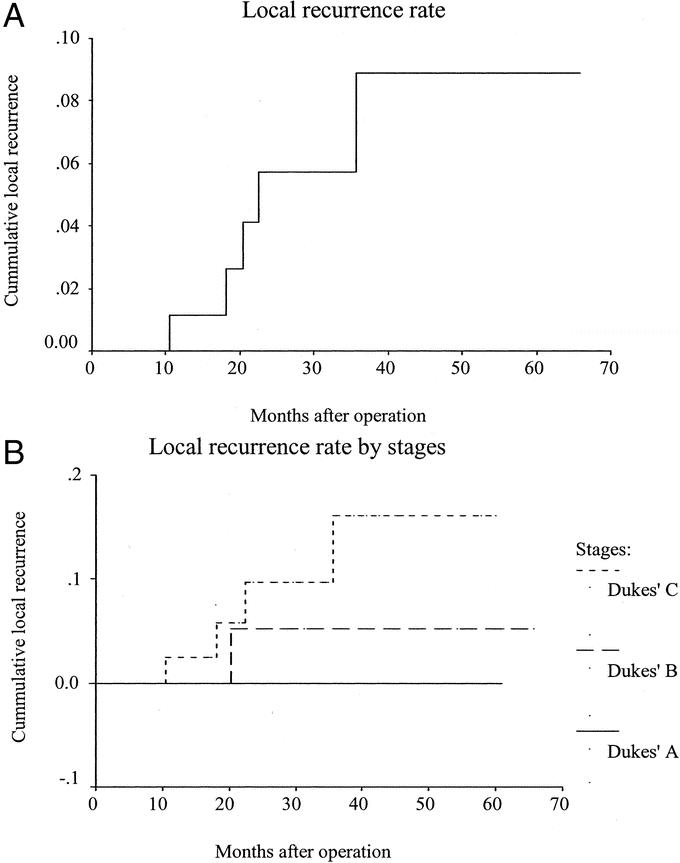
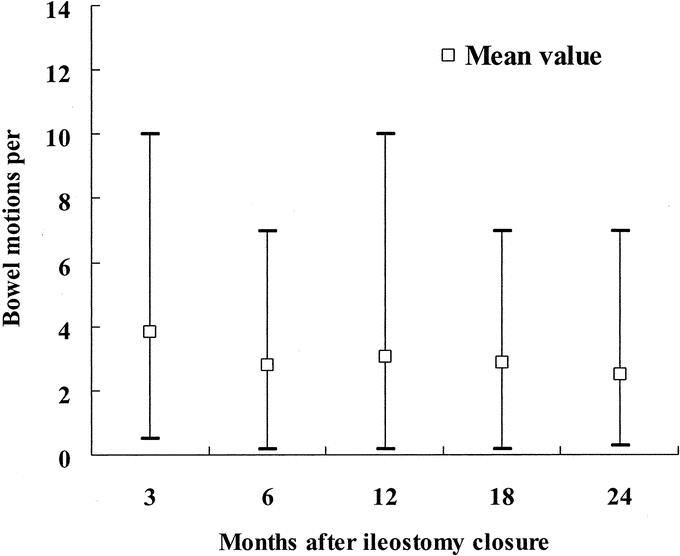
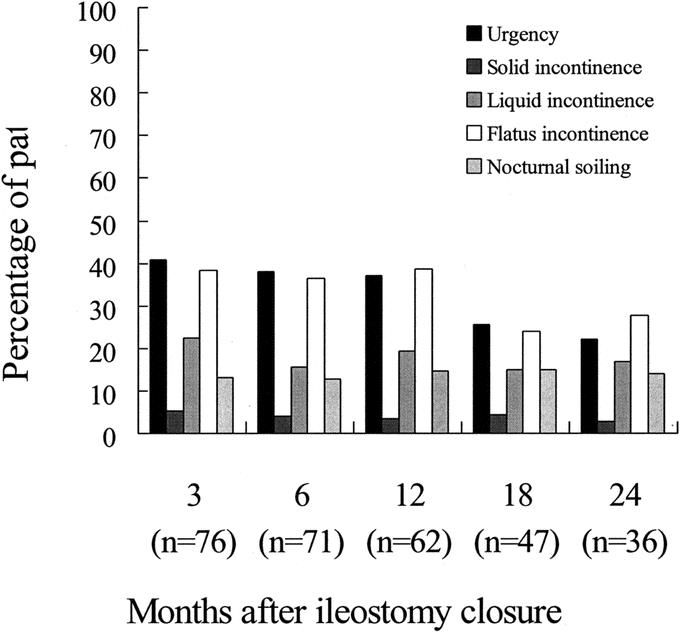
Results: From March 1999 to September 2004, 105 patients underwent laparoscopic TME with colonic J-pouch reconstruction. The mean operating time was 170.4 minutes and mean blood loss was 91.5 mL. The mean anastomotic distance from the anal verge was 3.9 cm. Conversion was required in 2 cases. The mean circumferential and distal margins were 17.1 mm and 3.4 cm, respectively. There was 1 case of microscopic circumferential margin involvement and 1 case of microscopic distal margin involvement. There was no 30-day mortality, and 6 patients underwent reoperation for major complications. There was no port-site metastasis. The mean follow-up time was 26.9 months (range, 1.3-65.6 months). The actuarial 5-year cancer-specific survival and local recurrence rates were 81.3% and 8.9%, respectively. Erectile dysfunction occurred in 13.6% of males, while 2 patients developed incomplete bladder denervation. Bowel function after ileostomy closure was satisfactory, with an average bowel motion of less than 3 times per day at 2 years after ileostomy closure.
Conclusions: Laparoscopic TME with colonic J-pouch reconstruction is a safe procedure with reasonable operating time and does not appear to pose any threat to the oncologic and functional outcomes.
Figures
References
-
- Jacobs M, Verdeja JC, Goldstein HS. Minimally invasive colon resection (laparoscopic colectomy). Surg Laparosc Endosc. 1991;1:144–150. - PubMed
-
- Leung KL, Kwok SPY, Lam SCW, et al. Laparoscopic resection of rectosigmoid cancer: prospective randomized trial. Lancet. 2004;363:1187–1192. - PubMed
-
- Clinical Outcomes of Surgical Therapy Study Group. A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med. 2004;350:2050–2059. - PubMed
-
- Lacy AM, Garcia-Valdecasas JC, Delgado S, et al. Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet. 2002;359:2224–2229. - PubMed
-
- Scheidbach H, Schneider C, Baerlehner E, et al. Laparoscopic anterior resection for rectal carcinoma: results of a registry. Surg Oncol Clin North Am. 2001;10:599–609. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
