

Burden of illness in bipolar depression
- PMID: 16498488
- PMCID: PMC1324957
- DOI: 10.4088/pcc.v07n0601
Burden of illness in bipolar depression
Abstract
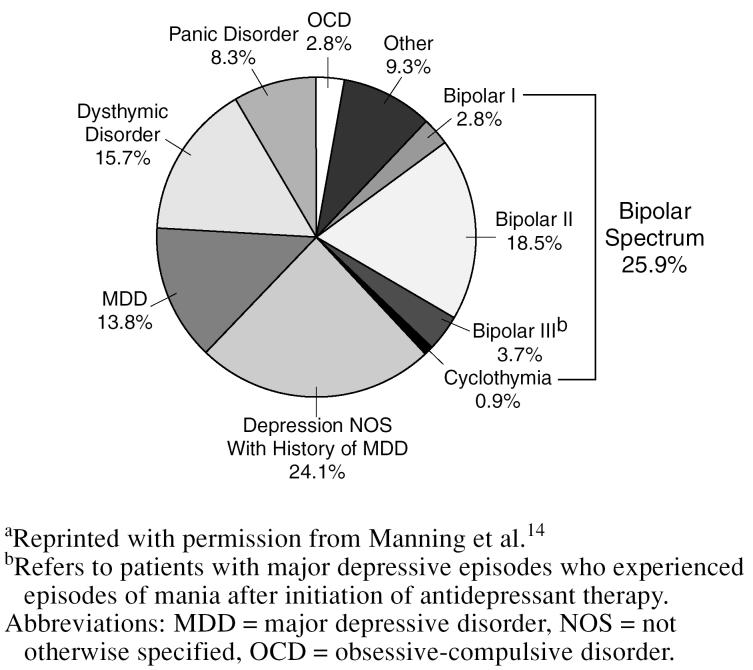
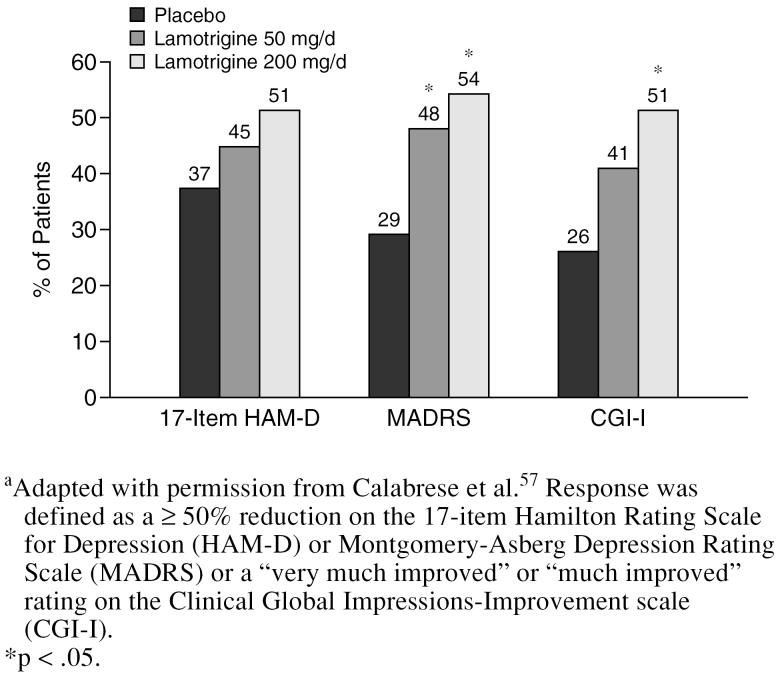
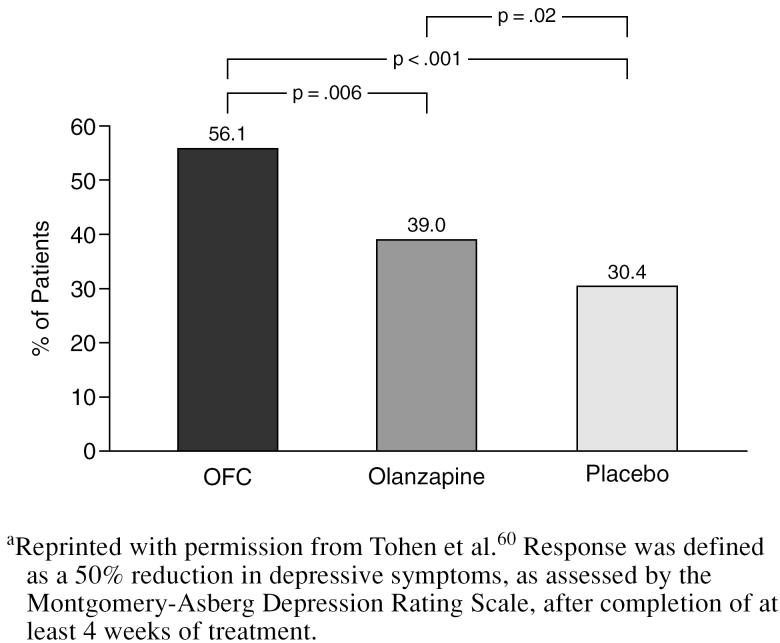
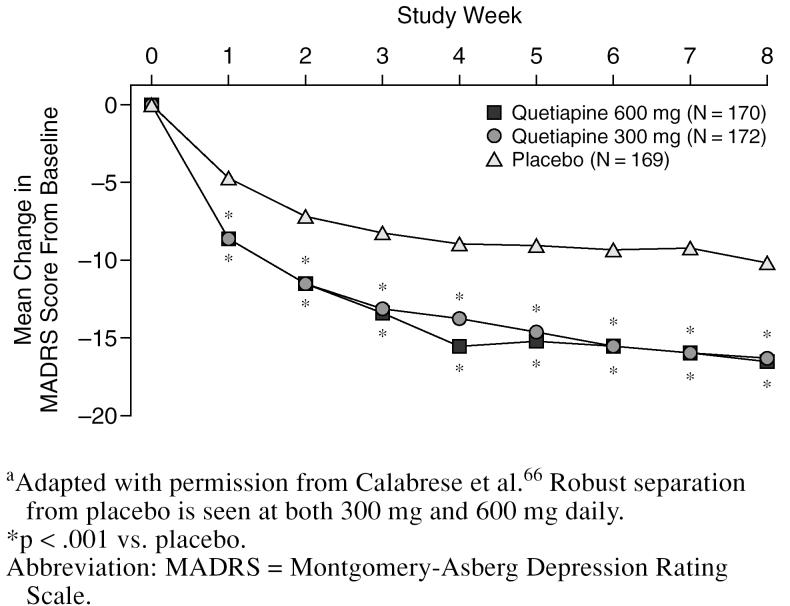
Bipolar depression is the underrecognized and unappreciated phase of bipolar disorder. Nevertheless, bipolar depression is responsible for much of the morbidity and mortality associated with the disorder. Depressive symptoms are far more prevalent than hypomanic or manic symptoms in bipolar patients, and they are associated with a heavier burden of illness, including reduced functioning, increased risk of suicidal acts, and high economic costs. Because most patients with bipolar disorder present with depression, misdiagnoses of major depressive disorder are common, even typical. Comorbid psychiatric disorders are also prevalent and may obscure the diagnosis and complicate treatment strategies. Depressed patients should be carefully assessed for manic or hypomanic symptoms to help reveal possible bipolar disorder. In addition to evaluation of psychiatric symptoms, a close examination of family history, course of illness, and treatment response will aid the clinician in making an accurate diagnosis. Treatment of acute depression in bipolar patients may require therapy combining agents such as lithium, divalproex, lamotrigine, carbamazepine, and atypical antipsychotics or using such agents in combination with an anti-depressant. Olanzapine/fluoxetine combination is the only medication currently approved for the treatment of bipolar depression. Antidepressant monotherapy should not be used, because there is evidence that such treatment increases the risk of switching into mania/hypomania and could induce treatment-refractory conditions such as mixed or rapid-cycling states. Maintenance therapy will be required by most patients, since discontinuation of mood stabilizers or antidepressants frequently leads to relapses in depressive symptoms. Prompt diagnosis and the use of specific therapeutic agents with evidence of efficacy may help reduce the disease burden associated with bipolar depression.
Figures
References
-
- Judd LL, Akiskal HS.. The prevalence and disability of bipolar spectrum disorders in the US population: re-analysis of the ECA database taking into account subthreshold cases. J Affect Disord. 2003;73:123–131. - PubMed
-
- ten Have M, Vollebergh W, and Bijl R. et al. Bipolar disorder in the general population in the Netherlands (prevalence, consequences and care utilisation): results from the Netherlands Mental Health Survey and Incidence Study (NEMESIS). J Affect Disord. 2002 68:203–213. - PubMed
-
- Kupfer DJ, Frank E, and Grochocinski VJ. et al. Demographic and clinical characteristics of individuals in a bipolar disorder case registry. J Clin Psychiatry. 2002 63:120–125. - PubMed
-
- Goetzel RZ, Hawkins K, and Ozminkowsky RJ. et al. The health and productivity cost burden of the “top 10” physical and mental health conditions affecting six large US employers in 1999. J Occup Environ Med. 2003 45:5–14. - PubMed
-
- Tondo L, Isacsson G, Baldessarini R.. Suicidal behavior in bipolar disorder: risk and prevention. CNS Drugs. 2003;17:491–511. - PubMed
LinkOut - more resources
Full Text Sources