

Cellular basis for electrocardiographic and arrhythmic manifestations of Andersen-Tawil syndrome (LQT7)
- PMID: 16500306
- PMCID: PMC1474110
- DOI: 10.1016/j.hrthm.2005.11.026
Cellular basis for electrocardiographic and arrhythmic manifestations of Andersen-Tawil syndrome (LQT7)
Abstract
Background: Andersen-Tawil syndrome, a skeletal muscle syndrome associated with periodic paralysis and long QT intervals on the ECG, has been linked to defects in KCNJ2, the gene encoding for the inward rectifier potassium channel (I(K1).)
Objectives: The purpose of this study was to examine the cellular mechanisms underlying the ECG and arrhythmic manifestations of Andersen-Tawil syndrome.
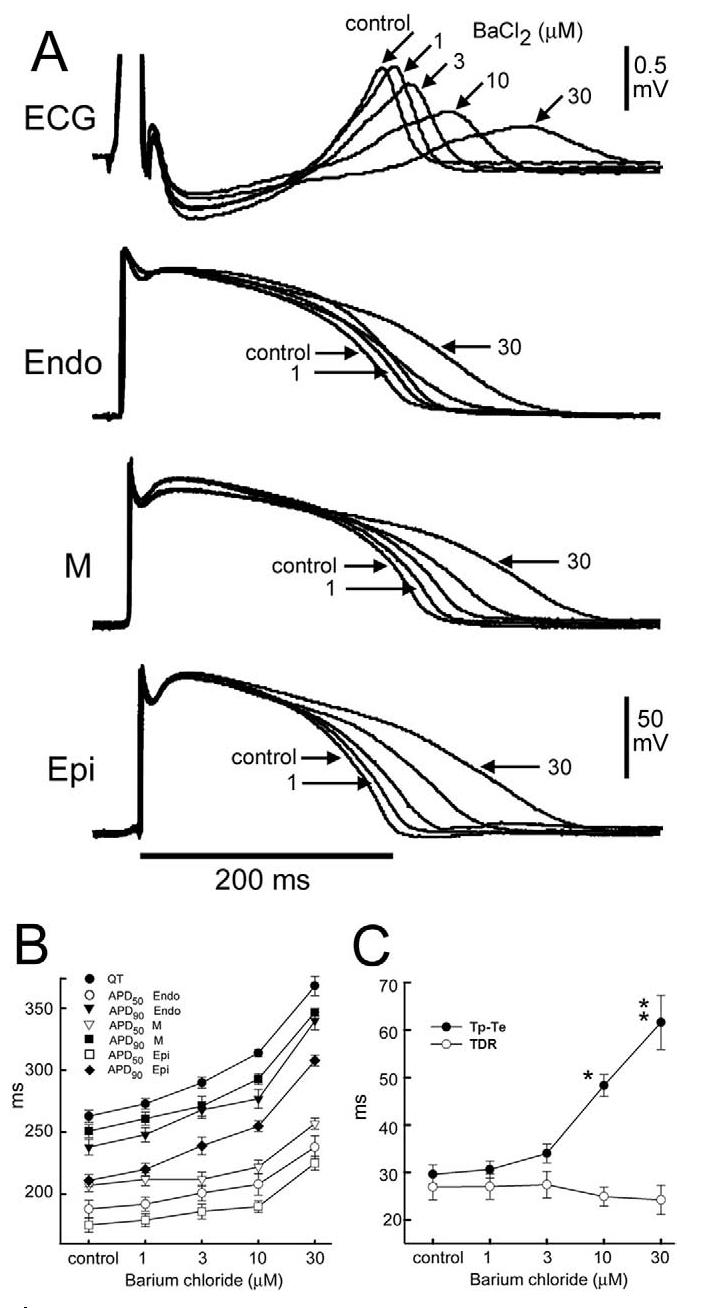
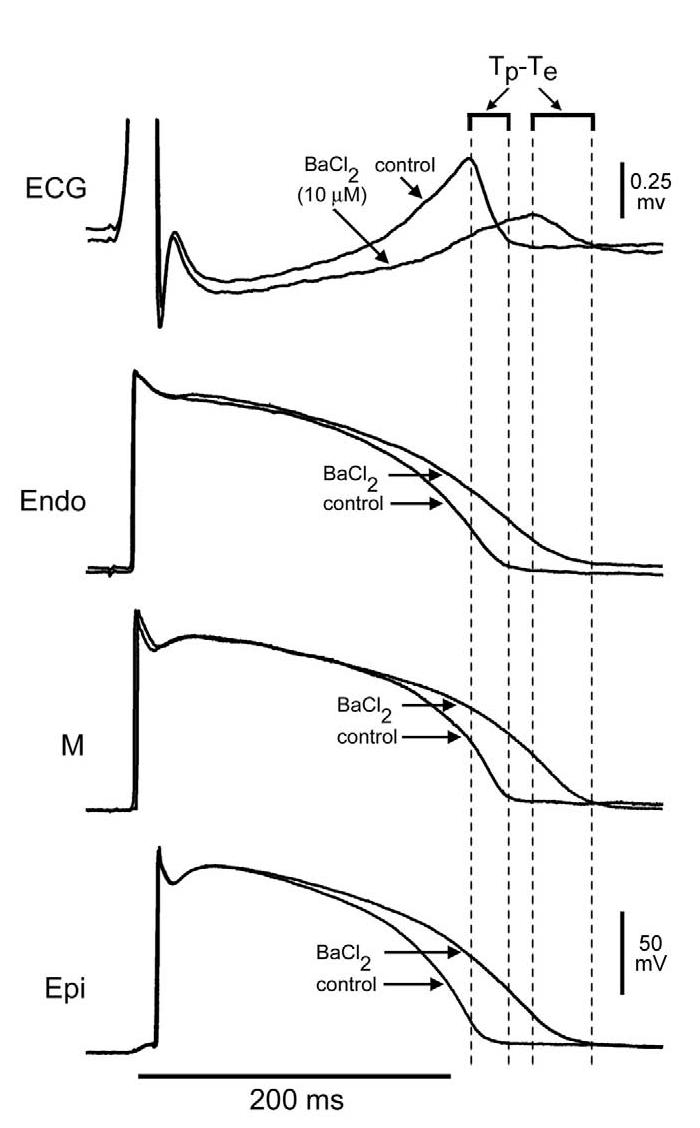
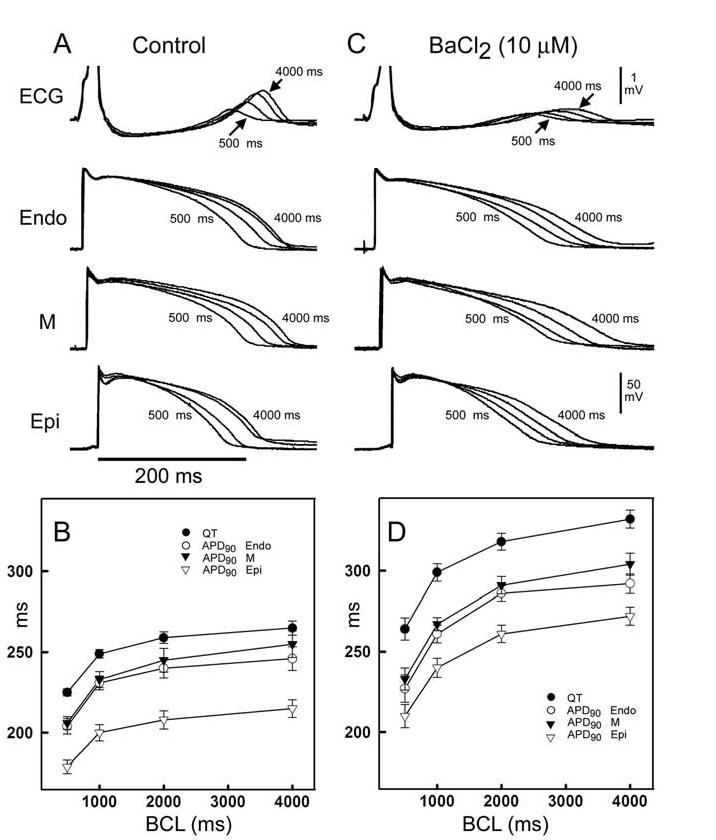
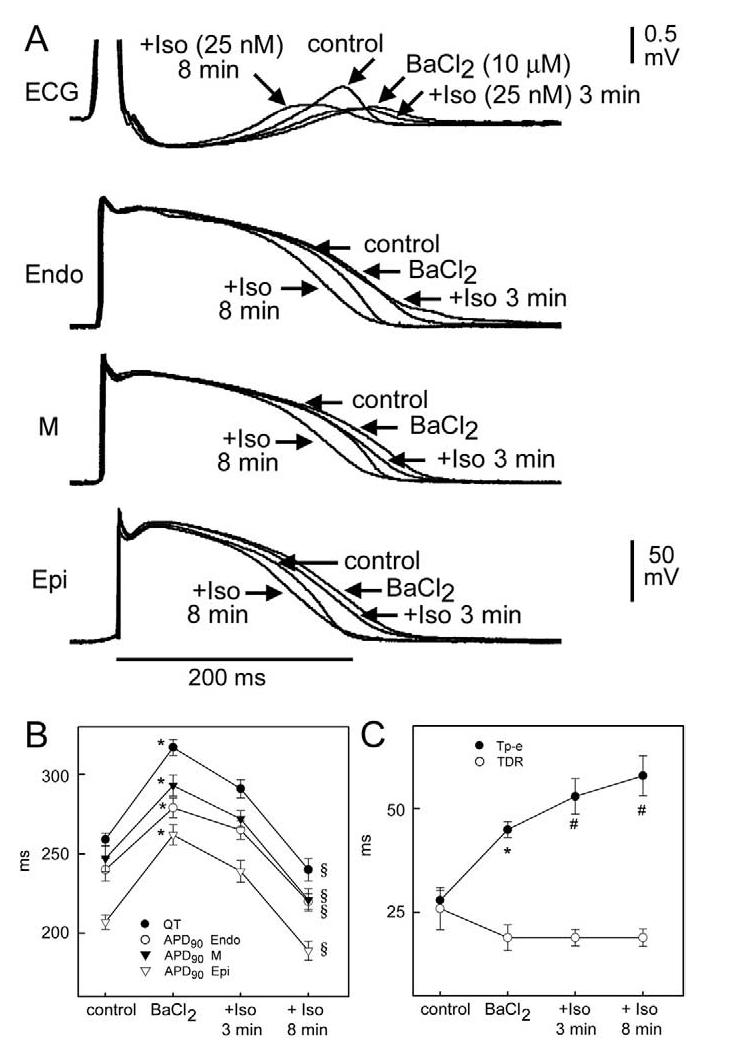
Methods: To investigate the effects of KCNJ2 loss-of-function mutations responsible for Andersen-Tawil syndrome, we used barium chloride (BaCl(2)) to inhibit I(K1) in arterially perfused wedge preparation. Transmembrane action potentials (APs) were simultaneously recorded from endocardial, midmyocardial, and epicardial cells, together with a transmural ECG.
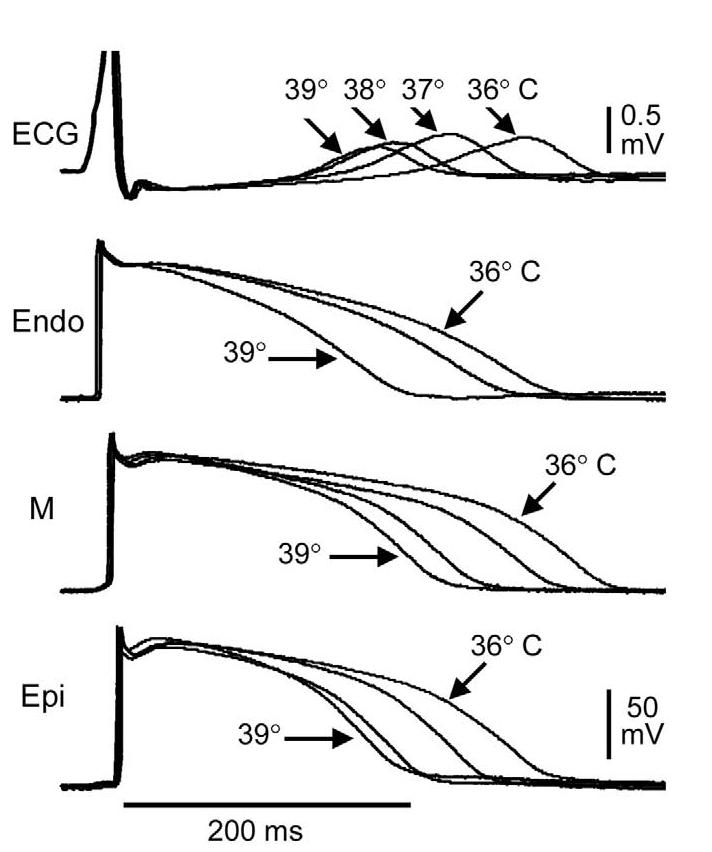
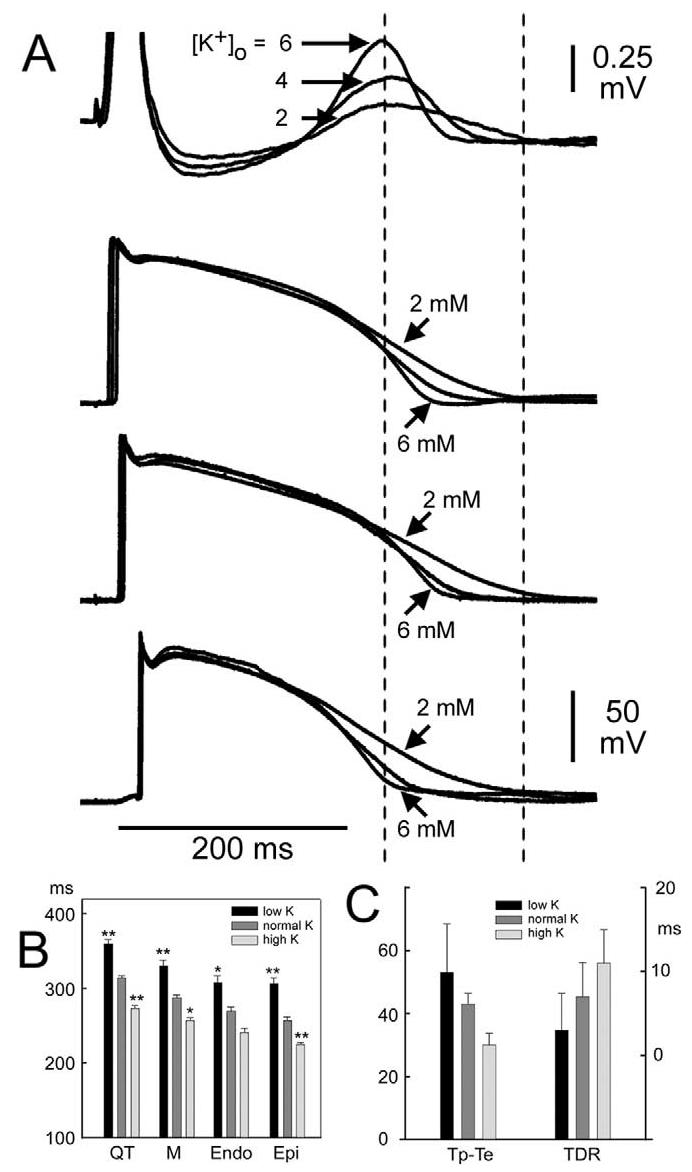
Results: BaCl(2) (1 to 30 microM) produced a concentration-dependent prolongation of the QT interval, secondary to a homogeneous prolongation of AP duration of the three cell types. QT interval was prolonged without an increase in transmural dispersion of repolarization (TDR). Low extracellular potassium (2.0 mM), isoproterenol (20-50 nM), and an abrupt increase in temperature (36 degrees C-39 degrees C) in the presence of 10 microM BaCl(2) did not significantly increase TDR but increased ectopic extrasystolic activity. Early afterdepolarizations were not observed under any condition. Spontaneous torsades de pointes arrhythmias were never observed, nor could they be induced with programmed electrical stimulation under any of the conditions studied.
Conclusion: Our results provide an understanding of why QT prolongation associated with Andersen-Tawil syndrome is relatively benign in the clinic and provide further support for the hypothesis that the increase in TDR, rather than QT interval, is responsible for development of torsades de pointes.
Figures
Comment in
-
IK1: the long and the short QT of it.Heart Rhythm. 2006 Mar;3(3):336-8. doi: 10.1016/j.hrthm.2005.12.026. Heart Rhythm. 2006. PMID: 16500307 No abstract available.
Similar articles
-
Electrophysiological mechanisms of ventricular arrhythmias in relation to Andersen-Tawil syndrome under conditions of reduced IK1: a simulation study.Am J Physiol Heart Circ Physiol. 2006 Dec;291(6):H2597-605. doi: 10.1152/ajpheart.00393.2006. Epub 2006 Jul 28. Am J Physiol Heart Circ Physiol. 2006. PMID: 16877549
-
Heterogeneous ventricular chamber response to hypokalemia and inward rectifier potassium channel blockade underlies bifurcated T wave in guinea pig.Am J Physiol Heart Circ Physiol. 2007 Jun;292(6):H3043-51. doi: 10.1152/ajpheart.01312.2006. Epub 2007 Feb 16. Am J Physiol Heart Circ Physiol. 2007. PMID: 17307991
-
Sodium pentobarbital reduces transmural dispersion of repolarization and prevents torsades de Pointes in models of acquired and congenital long QT syndrome.J Cardiovasc Electrophysiol. 1999 Feb;10(2):154-64. doi: 10.1111/j.1540-8167.1999.tb00656.x. J Cardiovasc Electrophysiol. 1999. PMID: 10090218
-
Electrocardiogram in Andersen-Tawil syndrome. New electrocardiographic criteria for diagnosis of type-1 Andersen-Tawil syndrome.Curr Cardiol Rev. 2014 Aug;10(3):222-8. doi: 10.2174/1573403x10666140514102528. Curr Cardiol Rev. 2014. PMID: 24827800 Free PMC article. Review.
-
Andersen-Tawil syndrome: clinical and molecular aspects.Int J Cardiol. 2013 Dec 5;170(1):1-16. doi: 10.1016/j.ijcard.2013.10.010. Int J Cardiol. 2013. PMID: 24383070 Review.
Cited by
-
Molecular and genetic basis of sudden cardiac death.J Clin Invest. 2013 Jan;123(1):75-83. doi: 10.1172/JCI62928. Epub 2013 Jan 2. J Clin Invest. 2013. PMID: 23281413 Free PMC article. Review.
-
Novel mutation in the KCNJ2 gene is associated with a malignant arrhythmic phenotype of Andersen-Tawil syndrome.Ann Noninvasive Electrocardiol. 2013 Sep;18(5):471-8. doi: 10.1111/anec.12074. Ann Noninvasive Electrocardiol. 2013. PMID: 24047492 Free PMC article.
-
Mutational consequences of aberrant ion channels in neurological disorders.J Membr Biol. 2014 Nov;247(11):1083-127. doi: 10.1007/s00232-014-9716-2. Epub 2014 Aug 14. J Membr Biol. 2014. PMID: 25119057 Review.
-
Mechanisms Underlying the Actions of Antidepressant and Antipsychotic Drugs That Cause Sudden Cardiac Arrest.Arrhythm Electrophysiol Rev. 2018 Aug;7(3):199-209. doi: 10.15420/aer.2018.29.2. Arrhythm Electrophysiol Rev. 2018. PMID: 30416734 Free PMC article. Review.
-
Genetics of channelopathies associated with sudden cardiac death.Glob Cardiol Sci Pract. 2015 Oct 13;2015(3):39. doi: 10.5339/gcsp.2015.39. eCollection 2015. Glob Cardiol Sci Pract. 2015. PMID: 26566530 Free PMC article. Review.
References
-
- Plaster NM, Tawil R, Tristani-Firouzi M, Canun S, Bendahhou S, Tsunoda A, Donaldson MR, Iannaccone ST, Brunt E, Barohn R, Clark J, Deymeer F, George AL, Fish FA, Hahn A, Nitu A, Ozdemir C, Serdaroglu P, Subramony SH, Wolfe G, Fu YH, Ptacek LJ. Mutations in Kir2.1 cause the developmental and episodic electrical phenotypes of Andersen's syndrome. Cell. 2001;105:511–519. - PubMed
-
- Tristani-Firouzi M, Jensen JL, Donaldson MR, Sansone V, Meola G, Hahn A, Bendahhou S, Kwiecinski H, Fidzianska A, Plaster N, Fu YH, Ptacek LJ, Tawil R. Functional and clinical characterization of KCNJ2 mutations associated with LQT7 (Andersen syndrome) J Clin Invest. 2002;110:381–388. - PMC - PubMed
-
- Donaldson MR, Jensen JL, Tristani-Firouzi M, Tawil R, Bendahhou S, Suarez WA, Cobo AM, Poza JJ, Behr E, Wagstaff J, Szepetowski P, Pereira S, Mozaffar T, Escolar DM, Fu YH, Ptacek LJ. PIP2 binding residues of Kir2.1 are common targets of mutations causing Andersen syndrome. Neurology. 2003;60:1811–1816. - PubMed
-
- Ai T, Fujiwara Y, Tsuji K, Otani H, Nakano S, Kubo Y, Horie M. Novel KCNJ2 mutation in familial periodic paralysis with ventricular dysrhythmia. Circulation. 2002;105:2592–2594. - PubMed
-
- Hosaka Y, Hanawa H, Washizuka T, Chinushi M, Yamashita F, Yoshida T, Komura S, Watanabe H, Aizawa Y. Function, subcellular localization and assembly of a novel mutation of KCNJ2 in Andersen's syndrome. J Mol Cell Cardiol. 2003;35:409–415. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
