

Developing a prioritisation framework in an English Primary Care Trust
- PMID: 16503989
- PMCID: PMC1395334
- DOI: 10.1186/1478-7547-4-3
Developing a prioritisation framework in an English Primary Care Trust
Abstract
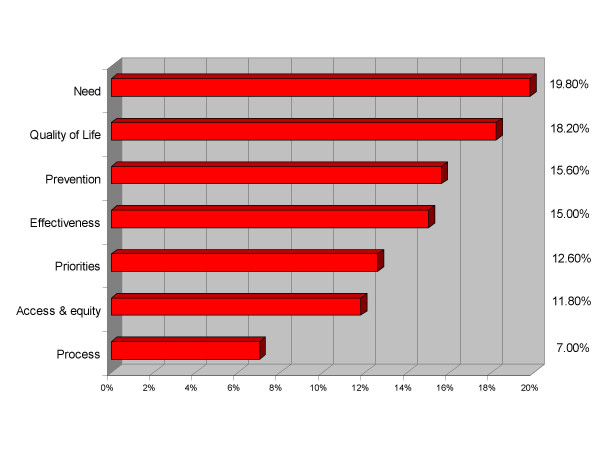
Background: In the English NHS, Primary Care Trusts (PCTs) are required to commission health services, to maximise the well-being of the population, subject to the available budget. There are numerous techniques employed to make decisions, some more rational and transparent than others. A weighted benefit score can be used to rank options but this does not take into account value for money from investments.
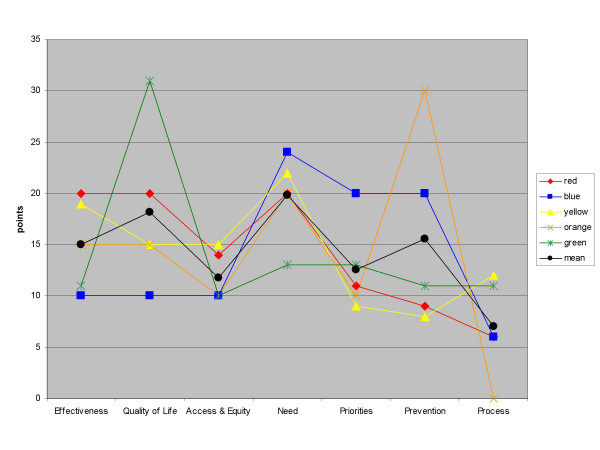
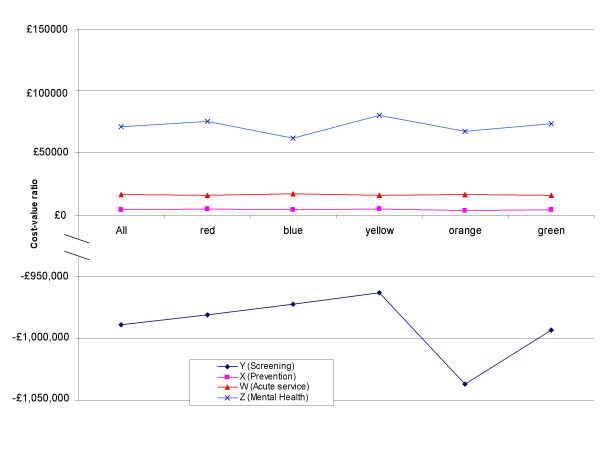
Methods: We developed a weighted benefit score framework for use in an English PCT which ranked options in order of 'cost-value' or 'cost per point of benefit'. Our method differs from existing techniques by explicitly combining cost and a composite weighted benefit score into the cost-value ratio.
Results: The technique proved readily workable, and was able to accommodate a wide variety of data and competing criteria. Participants felt able to assign scores to proposed services, and generate a ranked list, which provides a solid starting point for the PCT Board to discuss and make funding decisions. Limitations included potential for criteria to be neither exhaustive nor mutually exclusive and the lack of an interval property in the benefit score limiting the usefulness of a cost-value ratio.
Conclusion: A technical approach to decision making is insufficient for making prioritisation decisions, however our technique provides a very valuable, structured and informed starting point for PCT decision making.
Figures
Similar articles
-
Prioritizing health technologies in a Primary Care Trust.J Health Serv Res Policy. 2007 Apr;12(2):80-5. doi: 10.1258/135581907780279495. J Health Serv Res Policy. 2007. PMID: 17407656
-
Using programme budgeting and marginal analysis (PBMA) to set priorities: reflections from a qualitative assessment in an English Primary Care Trust.Soc Sci Med. 2013 Dec;98:162-8. doi: 10.1016/j.socscimed.2013.09.020. Epub 2013 Oct 2. Soc Sci Med. 2013. PMID: 24331895
-
A Framework to Prioritise Health Research Proposals for Funding: Integrating Value for Money.Appl Health Econ Health Policy. 2019 Dec;17(6):761-770. doi: 10.1007/s40258-019-00495-2. Appl Health Econ Health Policy. 2019. PMID: 31257553
-
Contextual Factors Influencing Cost and Quality Decisions in Health and Care: A Structured Evidence Review and Narrative Synthesis.Int J Health Policy Manag. 2018 Aug 1;7(8):683-695. doi: 10.15171/ijhpm.2018.09. Int J Health Policy Manag. 2018. PMID: 30078288 Free PMC article. Review.
-
Prioritisation of health technology assessment. The PATHS model: methods and case studies.Health Technol Assess. 2003;7(20):iii, 1-82. doi: 10.3310/hta7200. Health Technol Assess. 2003. PMID: 13678549 Review.
Cited by
-
Priority setting of health interventions: the need for multi-criteria decision analysis.Cost Eff Resour Alloc. 2006 Aug 21;4:14. doi: 10.1186/1478-7547-4-14. Cost Eff Resour Alloc. 2006. PMID: 16923181 Free PMC article.
-
Individual and societal effects of mental disorders on earnings in the United States: results from the national comorbidity survey replication.Am J Psychiatry. 2008 Jun;165(6):703-11. doi: 10.1176/appi.ajp.2008.08010126. Epub 2008 May 7. Am J Psychiatry. 2008. PMID: 18463104 Free PMC article.
-
'Real-world' health care priority setting using explicit decision criteria: a systematic review of the literature.BMC Health Serv Res. 2015 Apr 17;15:164. doi: 10.1186/s12913-015-0814-3. BMC Health Serv Res. 2015. PMID: 25927636 Free PMC article.
-
Eliciting preferences for reimbursed drugs selection criteria in Côte d'Ivoire.Patient. 2011;4(2):125-31. doi: 10.2165/11586060-000000000-00000. Patient. 2011. PMID: 21766901
-
Determining the Value of Two Biologic Drugs for Chronic Inflammatory Skin Diseases: Results of a Multi-Criteria Decision Analysis.BioDrugs. 2018 Jun;32(3):281-291. doi: 10.1007/s40259-018-0284-3. BioDrugs. 2018. PMID: 29808418 Free PMC article.
References
-
- Department of Health About us: The Department of Health. 2006. http://www.dh.gov.uk/AboutUs/fs/en
-
- Mitton C, Donaldson C. Priority Setting Toolkit: A guide to the use of economics in healthcare decision making. London, UK: BMJ Publishing; 2004. "Non-economic" approaches to priority setting; pp. 35–45.
-
- Edwards D, Peacock S, Carter R. Setting Priorities in South Australian Community Health III: Regional Applications of Program Budgeting and Marginal Analysis. Victoria, Australia: Centre for Health Program Evaluation; 1998. http://www.buseco.monash.edu.au/centres/che/pubs/rr15.pdf
LinkOut - more resources
Full Text Sources
