

Neonatal hearing screening: modelling cost and effectiveness of hospital- and community-based screening
- PMID: 16504089
- PMCID: PMC1402282
- DOI: 10.1186/1472-6963-6-14
Neonatal hearing screening: modelling cost and effectiveness of hospital- and community-based screening
Abstract
Background: Children with congenital hearing impairment benefit from early detection and management of their hearing loss. These and related considerations led to the recommendation of universal newborn hearing screening. In 2001 the first phase of a national Newborn Hearing Screening Programme (NHSP) was implemented in England. Objective of this study was to assess costs and effectiveness for hospital and community-based newborn hearing screening systems in England based on data from this first phase with regard to the effects of alterations to parameter values.
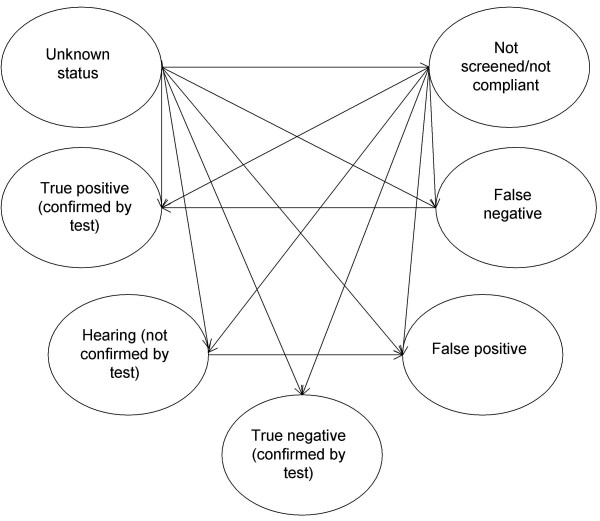
Design: Clinical effectiveness analysis using a Markov Model.
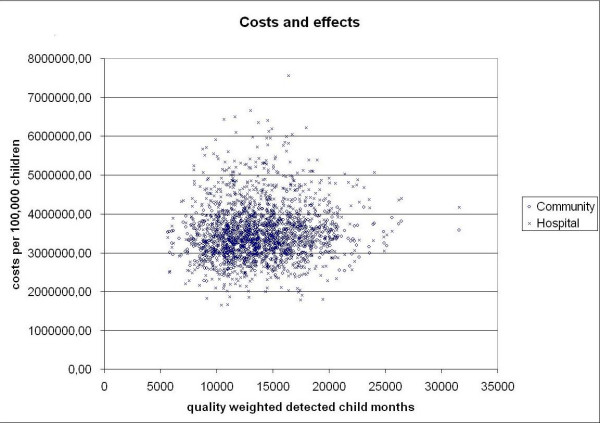
Outcome measure: quality weighted detected child months (QCM).
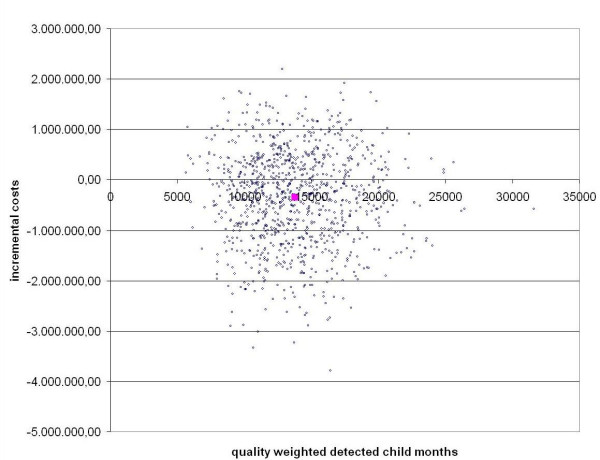
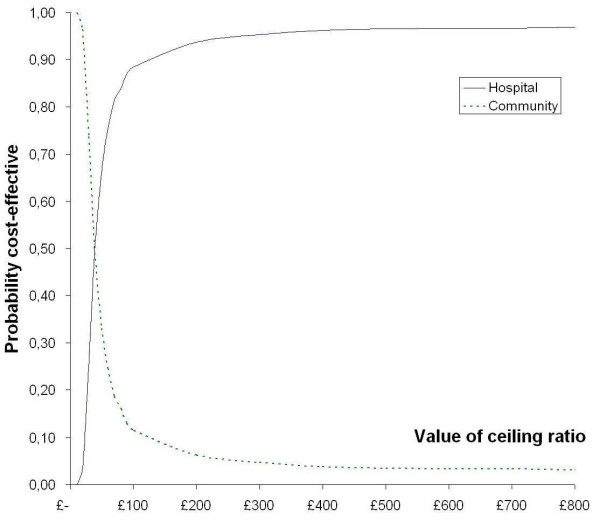
Results: Both hospital and community programmes yielded 794 QCM at the age of 6 months with total costs of 3,690,000 pound sterling per 100,000 screened children in hospital and 3,340,000 pound sterling in community. Simulated costs would be lower in hospital in 48% of the trials. Any statistically significant difference between hospital and community in prevalence, test sensitivity, test specificity and costs would result in significant differences in cost-effectiveness between hospital and community.
Conclusion: This modelling exercise informs decision makers by a quantitative projection of available data and the explicit and transparent statements about assumptions and the degree of uncertainty. Further evaluation of the cost-effectiveness should focus on the potential differences in test parameters and prevalence in these two settings.
Figures
References
-
- Fortnum H, Davis A. Epidemiology of permanent childhood hearing impairment in Trent Region. 1985-1993. Br J Audiol. 1997;31:409–446. - PubMed
-
- Parving A, Hauch AM. Permanent childhood hearing impairment - some cross-sectional characteristics from a surveillance program. International Pediatrics. 2001;16:1–5.
-
- Markides A. Age at fitting of hearing aids and speech intellegibility. Br J Audiol. 1986;20:165–167. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
