

Comparison of evidence on harms of medical interventions in randomized and nonrandomized studies
- PMID: 16505459
- PMCID: PMC1389826
- DOI: 10.1503/cmaj.050873
Comparison of evidence on harms of medical interventions in randomized and nonrandomized studies
Abstract
Background: Information on major harms of medical interventions comes primarily from epidemiologic studies performed after licensing and marketing. Comparison with data from large-scale randomized trials is occasionally feasible. We compared evidence from randomized trials with that from epidemiologic studies to determine whether they give different estimates of risk for important harms of medical interventions.
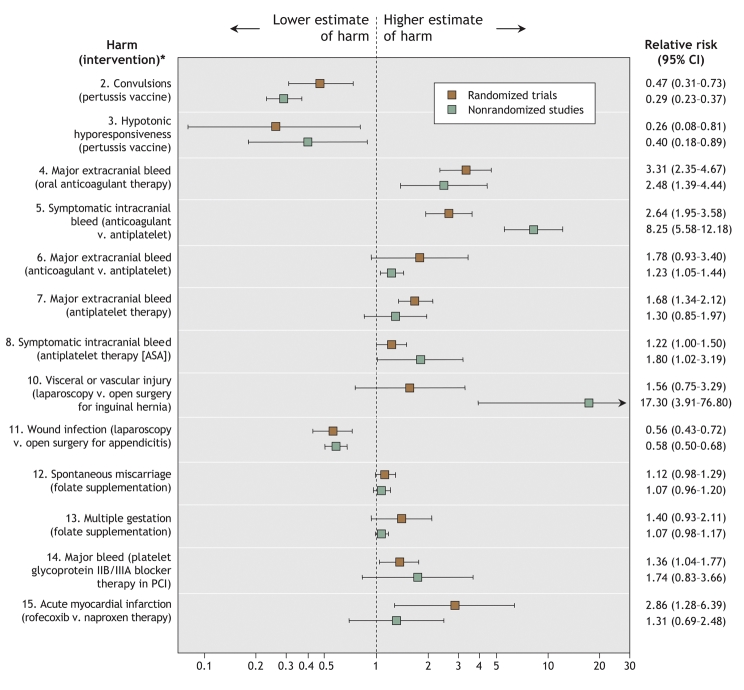
Methods: We targeted well-defined, specific harms of various medical interventions for which data were already available from large-scale randomized trials (> 4000 subjects). Nonrandomized studies involving at least 4000 subjects addressing these same harms were retrieved through a search of MEDLINE. We compared the relative risks and absolute risk differences for specific harms in the randomized and nonrandomized studies.
Results: Eligible nonrandomized studies were found for 15 harms for which data were available from randomized trials addressing the same harms. Comparisons of relative risks between the study types were feasible for 13 of the 15 topics, and of absolute risk differences for 8 topics. The estimated increase in relative risk differed more than 2-fold between the randomized and nonrandomized studies for 7 (54%) of the 13 topics; the estimated increase in absolute risk differed more than 2-fold for 5 (62%) of the 8 topics. There was no clear predilection for randomized or nonrandomized studies to estimate greater relative risks, but usually (75% [6/8]) the randomized trials estimated larger absolute excess risks of harm than the nonrandomized studies did.
Interpretation: Nonrandomized studies are often conservative in estimating absolute risks of harms. It would be useful to compare and scrutinize the evidence on harms obtained from both randomized and nonrandomized studies.
Figures
Comment in
-
What is the best evidence for determining harms of medical treatment?CMAJ. 2006 Feb 28;174(5):645-6. doi: 10.1503/cmaj.051484. CMAJ. 2006. PMID: 16505461 Free PMC article. No abstract available.
References
-
- Ioannidis JP, Lau J. Completeness of safety reporting in randomized trials: an evaluation of 7 medical areas. JAMA 2001;285:437-43. - PubMed
-
- Ioannidis JP, Evans SJ, Gotzsche PC, et al; CONSORT Group. Better reporting of harms in randomized trials: an extension of the CONSORT statement. Ann Intern Med 2004;141:781-8. - PubMed
-
- Topol EJ. Failing the public health — rofecoxib, Merck, and the FDA. N Engl J Med 2004;351:1707-9. - PubMed
-
- Lasser KE, Allen PD, Woolhandler SJ, et al. Timing of new black box warnings and withdrawals for prescription medications. JAMA 2002;287:2215-20. - PubMed
-
- Jick H. The discovery of drug-induced illness. N Engl J Med 1977;296:481-5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources