

Echocardiographic assessment of subclinical left ventricular eccentric hypertrophy in adult-onset GHD patients by geometric remodeling: an observational case-control study
- PMID: 16507109
- PMCID: PMC1483822
- DOI: 10.1186/1472-6823-6-1
Echocardiographic assessment of subclinical left ventricular eccentric hypertrophy in adult-onset GHD patients by geometric remodeling: an observational case-control study
Abstract
Background: Most patients with growth hormone deficiency (GHD) show high body mass index. Overweight subjects, but GHD patients, were demonstrated to have high left ventricular mass index (LVMi) and abnormal LV geometric remodeling. We sought to study these characteristics in a group of GHD patients, in an attempt to establish the BMI-independent role of GHD.
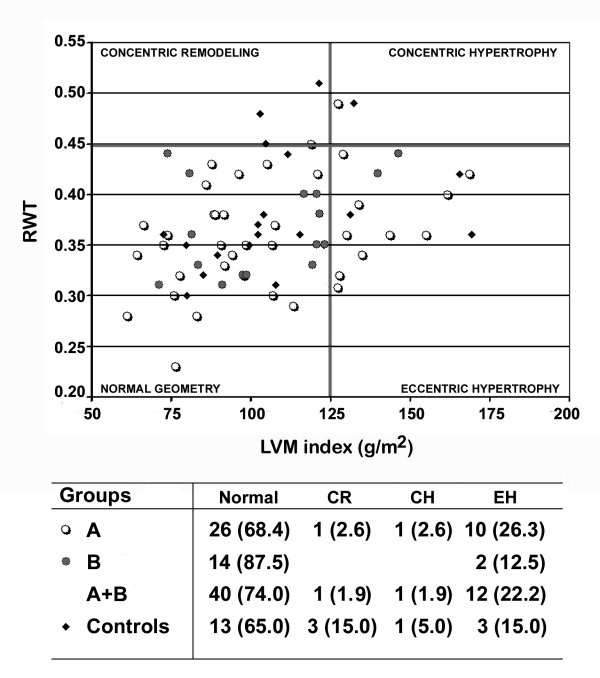
Methods: Fifty-four patients, 28 F and 26 M, aged 45.9 +/- 13.1, with adult-onset GHD (pituitary adenomas 48.2%, empty sella 27.8%, pituitary inflammation 5.5%, cranio-pharyngioma 3.7%, not identified pathogenesis 14.8%) were enrolled. To minimize any possible interferences of BMI on the aim of this study, the control group included 20 age- and weight-matched healthy subjects. The LV geometry was identified by the relationship between LVMi (cut-off 125 g/m2) and relative wall thickness (cut-off 0.45) at echocardiography.
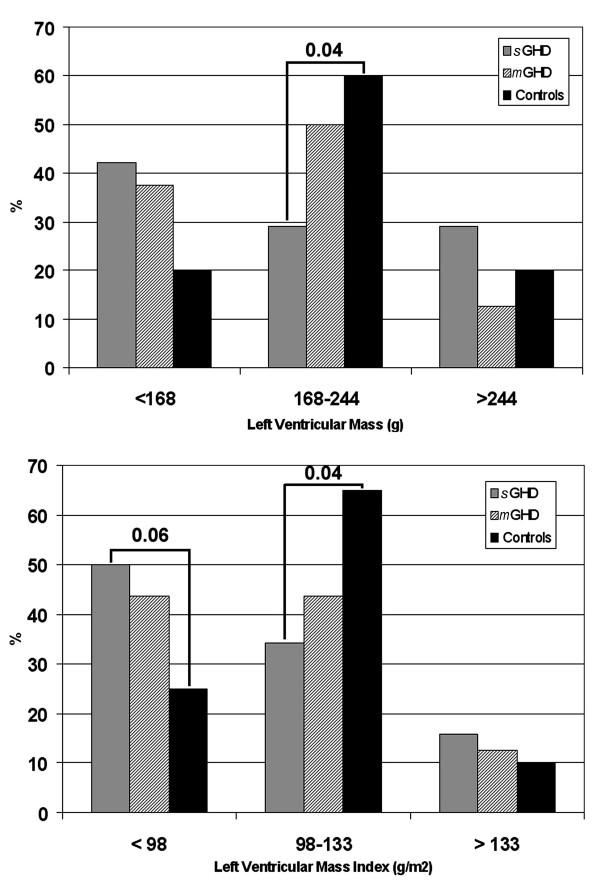
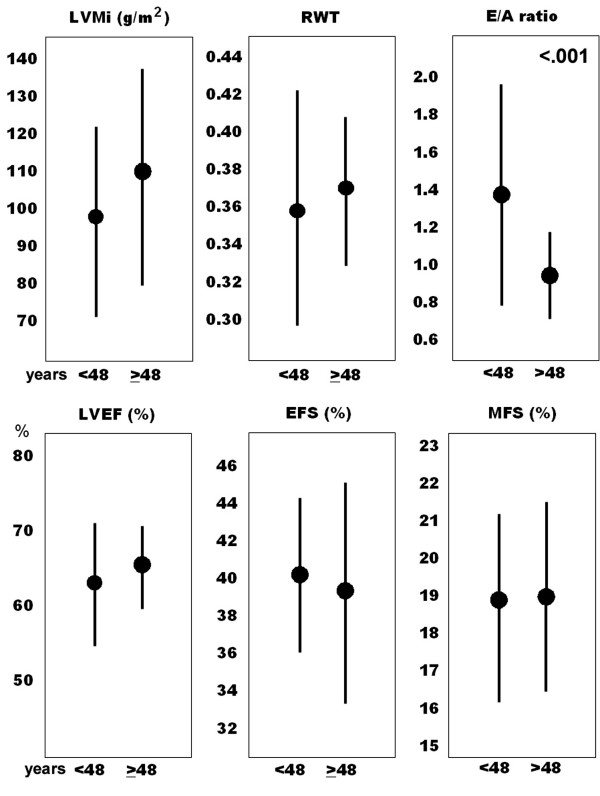
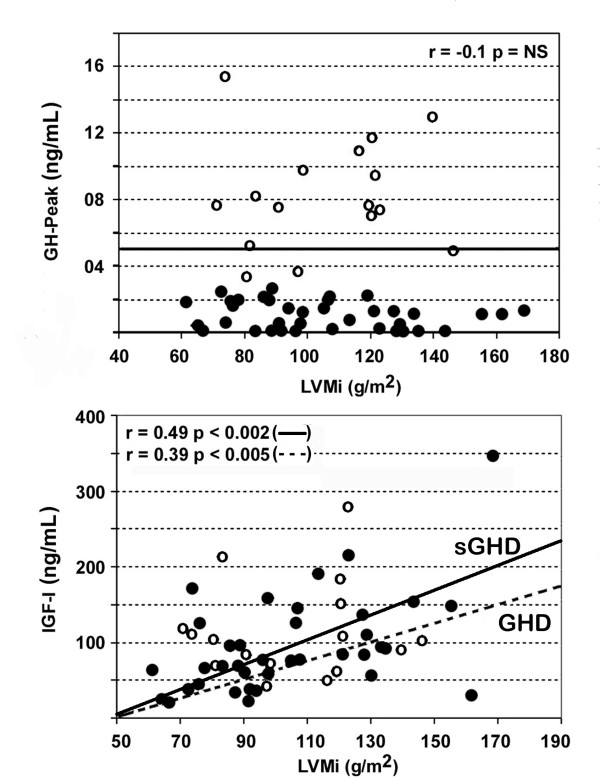
Results: There was no significant between-group difference in resting cardiac morphology and function, nor when considering age-related discrepancy. The majority of patients had normal-low LVM/LVMi, but about one fourth of them showed higher values. These findings correlated to relatively high circulating IGF-1 and systolic blood pressure at rest. The main LV geometric pattern was eccentric hypertrophy in 22% of GHD population (26% of with severe GHD) and in 15% of controls (p = NS).
Conclusion: Though the lack of significant differences in resting LV morphology and function, about 25% of GHD patients showed high LVMi (consisting of eccentric hypertrophy), not dissimilarly to overweight controls. This finding, which prognostic role is well known in obese and hypertensive patients, is worthy to be investigated in GHD patients through wider controlled trials.
Figures
References
-
- Amato G, Carella C, Fazio S, La Montagna G, Cittadini A, Sabatini D, Marciano-Mone C, Saccà L, Bellastella A. Body composition, bone metabolism, heart structure and function in growth hormone deficient adult before and after growth hormone replacement therapy at low doses. J Clin Endocrinol Metab. 1993;77:1671–1676. doi: 10.1210/jc.77.6.1671. - DOI - PubMed
-
- Carrol PV, Christ E, the members of Growth Hormone Research Society Scientific Committee. Bengtsson BA, Carlsson L, Christiansen JS, Clemmons D, Hintz R, Ho K, Laron Z, Sizonenko P, Sonksen PH, Tanaka T, Thorner M. Growth hormone deficiency in adulthood and the effects of growth hormone replacement: A review. J Clin Endocrinol Metab. 1998;83:382–395. doi: 10.1210/jc.83.2.382. - DOI - PubMed
-
- Jorgensen JOL, Muller J, Moller J, Wolthers T, Vahl N, Juul A, Skakkerbaek NE, Christiansen JS. Adult growth hormone deficiency. Horm Res. 1994;42:235–241. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
