

Lactate versus non-lactate metabolic acidosis: a retrospective outcome evaluation of critically ill patients
- PMID: 16507145
- PMCID: PMC1550830
- DOI: 10.1186/cc3987
Lactate versus non-lactate metabolic acidosis: a retrospective outcome evaluation of critically ill patients
Abstract
Introduction: Acid-base abnormalities are common in the intensive care unit (ICU). Differences in outcome exist between respiratory and metabolic acidosis in similar pH ranges. Some forms of metabolic acidosis (for example, lactate) seem to have worse outcomes than others (for example, chloride). The relative incidence of each type of disorder is unknown. We therefore designed this study to determine the nature and clinical significance of metabolic acidosis in critically ill patients.
Methods: An observational, cohort study of critically ill patients was performed in a tertiary care hospital. Critically ill patients were selected on the clinical suspicion of the presence of lactic acidosis. The inpatient mortality of the entire group was 14%, with a length of stay in hospital of 12 days and a length of stay in the ICU of 5.8 days.
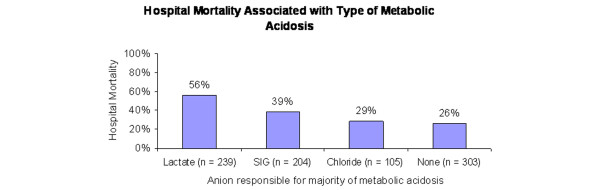
Results: We reviewed records of 9,799 patients admitted to the ICUs at our institution between 1 January 2001 and 30 June 2002. We selected a cohort in which clinicians caring for patients ordered a measurement of arterial lactate level. We excluded patients in which any necessary variable required to characterize an acid-base disorder was absent. A total of 851 patients (9% of ICU admissions) met our criteria. Of these, 548 patients (64%) had a metabolic acidosis (standard base excess < -2 mEq/l) and these patients had a 45% mortality, compared with 25% for those with no metabolic acidosis (p < 0.001). We then subclassified metabolic acidosis cases on the basis of the predominant anion present (lactate, chloride, or all other anions). The mortality rate was highest for lactic acidosis (56%); for strong ion gap (SIG) acidosis it was 39% and for hyperchloremic acidosis 29% (p < 0.001). A stepwise logistic regression model identified serum lactate, SIG, phosphate, and age as independent predictors of mortality.
Conclusion: In critically ill patients in which a measurement of lactate level was ordered, lactate and SIG were strong independent predictors of mortality when they were the major source of metabolic acidosis. Overall, patients with metabolic acidosis were nearly twice as likely to die as patients without metabolic acidosis.
Figures
Comment in
-
Causes and effects of hyperchloremic acidosis.Crit Care. 2006;10(3):413; author reply 413. doi: 10.1186/cc4963. Epub 2006 Jun 29. Crit Care. 2006. PMID: 16834765 Free PMC article. No abstract available.
References
-
- Balasubramanyan N, Havens PL, Hoffman GM. Unmeasured anions identified by the Fencl-Stewart method predict mortality better than base excess, anion gap, and lactate in patients in the pediatric intensive care unit. Crit Care Med. 1999;27:1577–1581. doi: 10.1097/00003246-199908000-00030. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
