

Thyroid status, cardiovascular risk, and mortality in older adults
- PMID: 16507804
- PMCID: PMC1387822
- DOI: 10.1001/jama.295.9.1033
Thyroid status, cardiovascular risk, and mortality in older adults
Abstract
Context: Previous studies have suggested that subclinical abnormalities in thyroid-stimulating hormone levels are associated with detrimental effects on the cardiovascular system.
Objective: To determine the relationship between baseline thyroid status and incident atrial fibrillation, incident cardiovascular disease, and mortality in older men and women not taking thyroid medication.
Design, setting, and participants: A total of 3233 US community-dwelling individuals aged 65 years or older with baseline serum thyroid-stimulating hormone levels were enrolled in 1989-1990 in the Cardiovascular Health Study, a large, prospective cohort study.
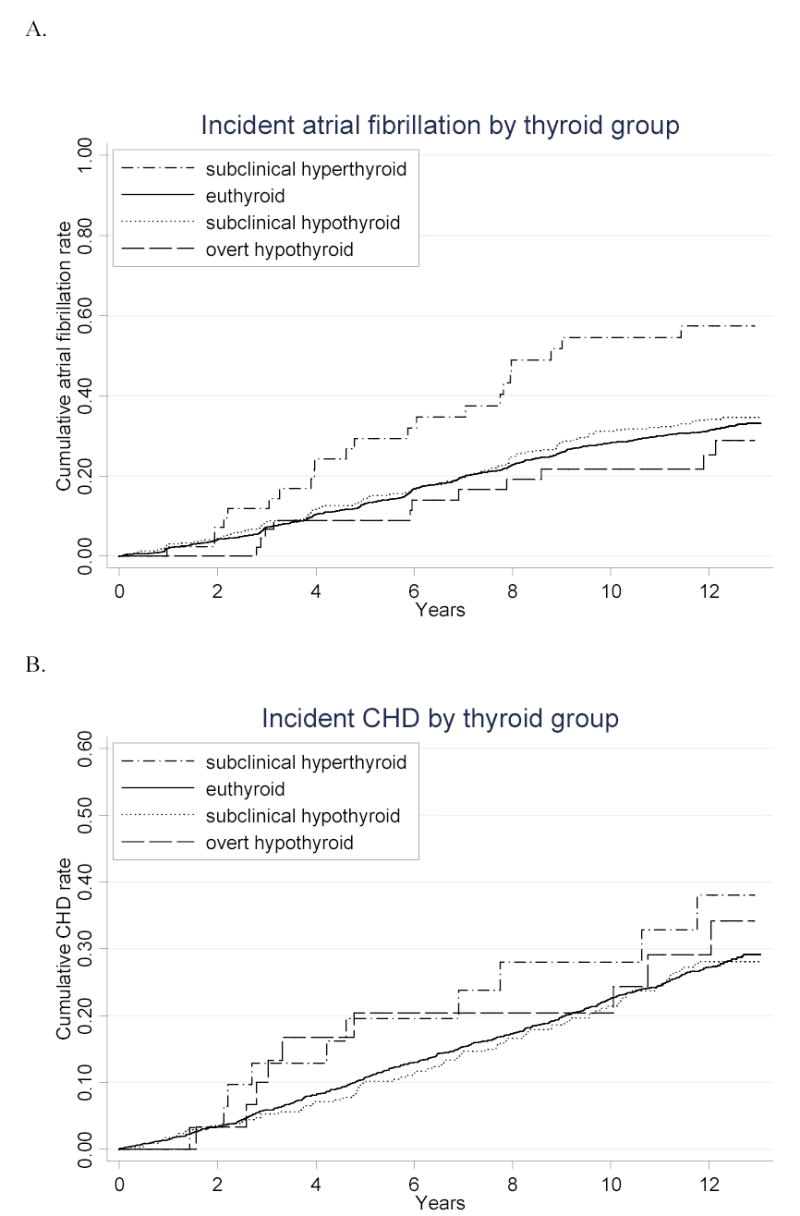
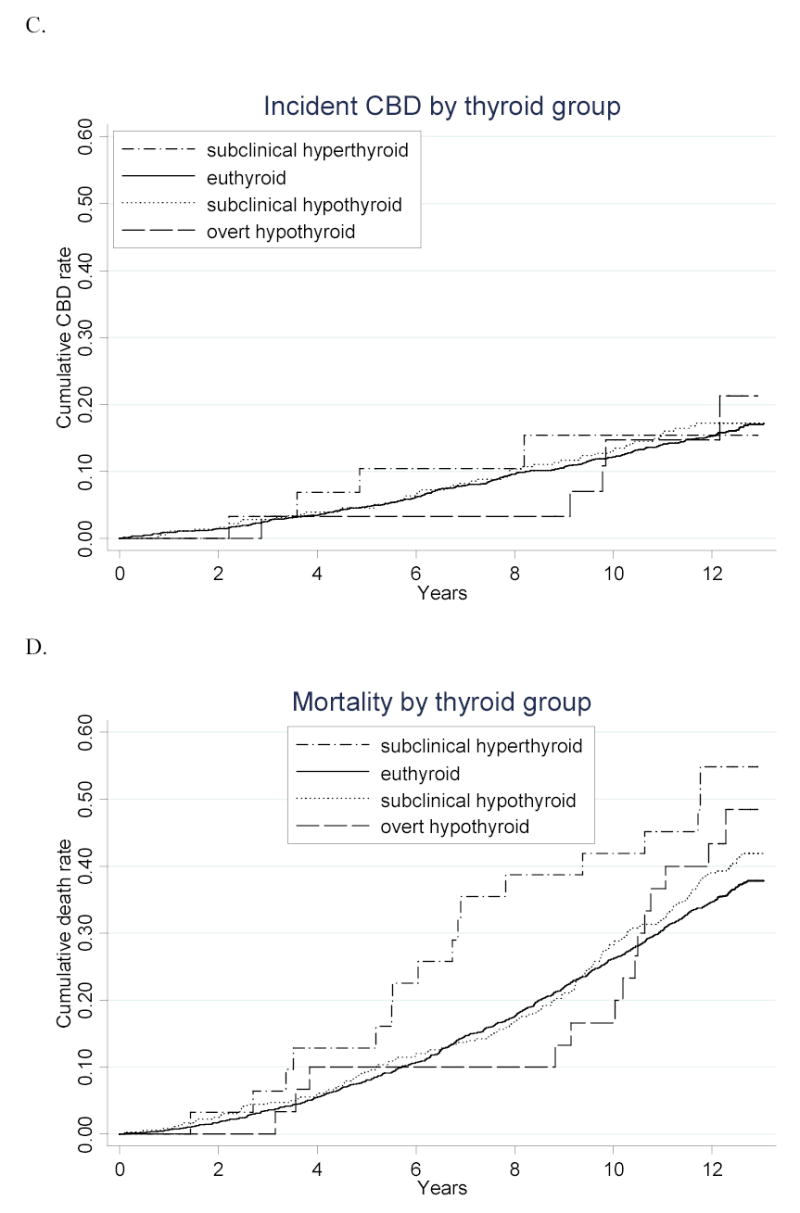
Main outcome measures: Incident atrial fibrillation, coronary heart disease, cerebrovascular disease, cardiovascular death, and all-cause death assessed through June 2002. Analyses are reported for 4 groups defined according to thyroid function test results: subclinical hyperthyroidism, euthyroidism, subclinical hypothyroidism, and overt hypothyroidism.
Results: Individuals with overt thyrotoxicosis (n = 4) were excluded because of small numbers. Eighty-two percent of participants (n = 2639) had normal thyroid function, 15% (n = 496) had subclinical hypothyroidism, 1.6% (n = 51) had overt hypothyroidism, and 1.5% (n = 47) had subclinical hyperthyroidism. After exclusion of those with prevalent atrial fibrillation, individuals with subclinical hyperthyroidism had a greater incidence of atrial fibrillation compared with those with normal thyroid function (67 events vs 31 events per 1000 person-years; adjusted hazard ratio, 1.98; 95% confidence interval, 1.29-3.03). No differences were seen between the subclinical hyperthyroidism group and euthyroidism group for incident coronary heart disease, cerebrovascular disease, cardiovascular death, or all-cause death. Likewise, there were no differences between the subclinical hypothyroidism or overt hypothyroidism groups and the euthyroidism group for cardiovascular outcomes or mortality. Specifically, individuals with subclinical hypothyroidism had an adjusted hazard ratio of 1.07 (95% confidence interval, 0.90-1.28) for incident coronary heart disease.
Conclusion: Our data show an association between subclinical hyperthyroidism and development of atrial fibrillation but do not support the hypothesis that unrecognized subclinical hyperthyroidism or subclinical hypothyroidism is associated with other cardiovascular disorders or mortality.
Figures
References
-
- Hoyert, DL, Kung HC, and Smith, BL. Deaths: Preliminary Data for 2003. National vital statistics reports. 53[15]. 2005. Hyattsville, Maryland, National Center for Health Statistics. - PubMed
-
- Magnus P, Beaglehole R. The real contribution of the major risk factors to the coronary epidemics: time to end the “only-50%” myth. Arch Intern Med. 2001;161:2657–2660. - PubMed
-
- Pahor M, Elam MB, Garrison RJ, Kritchevsky SB, Applegate WB. Emerging noninvasive biochemical measures to predict cardiovascular risk. Arch Intern Med. 1999;159:237–245. - PubMed
-
- Hak AE, Pols HA, Visser TJ, Drexhage HA, Hofman A, Witteman JC. Subclinical hypothyroidism is an independent risk factor for atherosclerosis and myocardial infarction in elderly women: the Rotterdam Study. Ann Intern Med. 2000;132:270–278. - PubMed
-
- Parle JV, Maisonneuve P, Sheppard MC, Boyle P, Franklyn JA. Prediction of all-cause and cardiovascular mortality in elderly people from one low serum thyrotropin result: a 10-year cohort study. Lancet. 2001;358:861–865. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K23 AG019161/AG/NIA NIH HHS/United States
- N01-HC-85085/HC/NHLBI NIH HHS/United States
- N01-HC-85081/HC/NHLBI NIH HHS/United States
- N01-HC-85086/HC/NHLBI NIH HHS/United States
- N01-HC-85082/HC/NHLBI NIH HHS/United States
- K23-AG19161/AG/NIA NIH HHS/United States
- N01-HC-85079/HC/NHLBI NIH HHS/United States
- N01 HC035129/HC/NHLBI NIH HHS/United States
- N01-HC-85084/HC/NHLBI NIH HHS/United States
- N01 HC015103/HC/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- N01-HC-85083/HC/NHLBI NIH HHS/United States
- N01-HC-85080/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
