

Therapeutic effects of xanthine oxidase inhibitors: renaissance half a century after the discovery of allopurinol
- PMID: 16507884
- PMCID: PMC2233605
- DOI: 10.1124/pr.58.1.6
Therapeutic effects of xanthine oxidase inhibitors: renaissance half a century after the discovery of allopurinol
Abstract
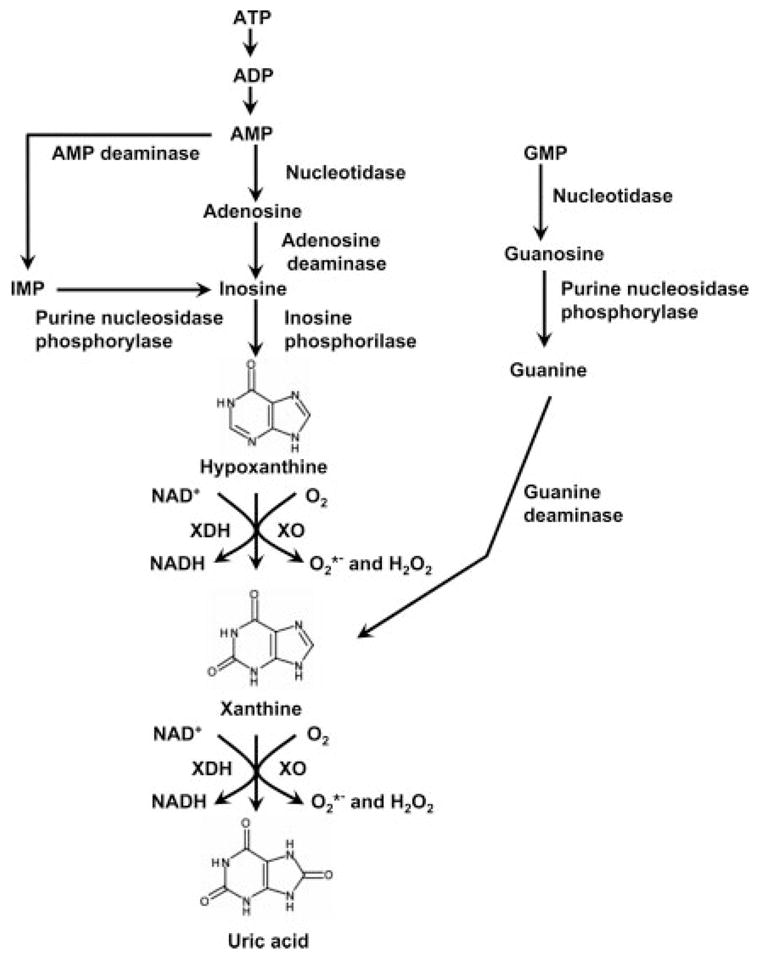
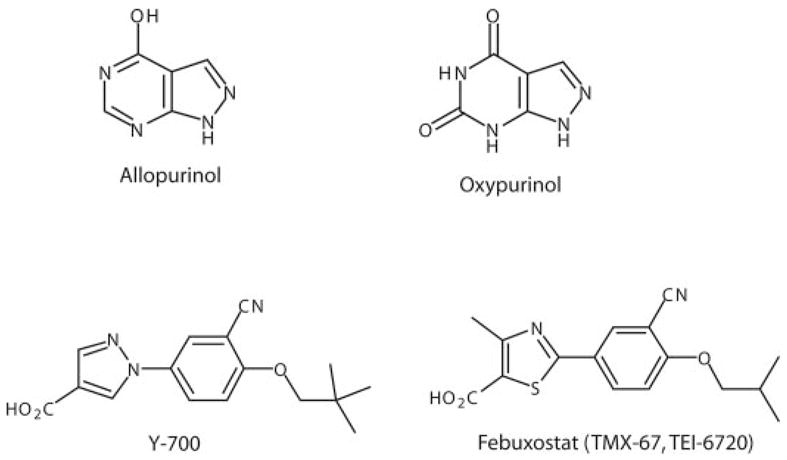
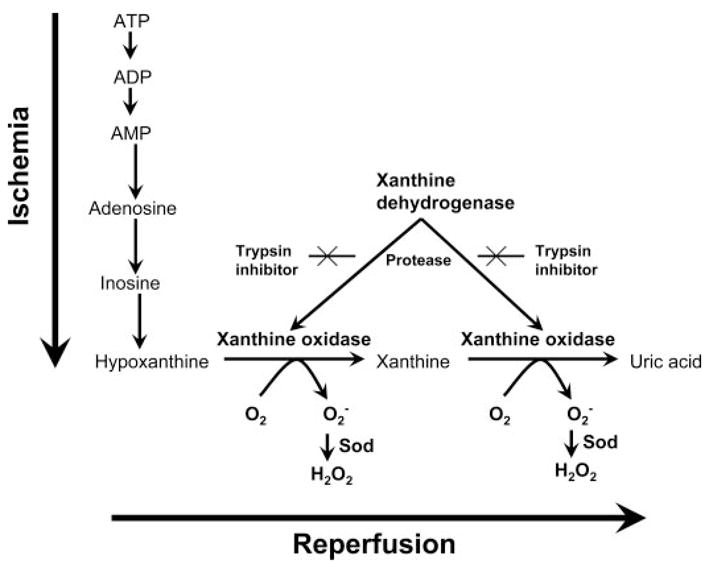
The prototypical xanthine oxidase (XO) inhibitor allopurinol, has been the cornerstone of the clinical management of gout and conditions associated with hyperuricemia for several decades. More recent data indicate that XO also plays an important role in various forms of ischemic and other types of tissue and vascular injuries, inflammatory diseases, and chronic heart failure. Allopurinol and its active metabolite oxypurinol showed considerable promise in the treatment of these conditions both in experimental animals and in small-scale human clinical trials. Although some of the beneficial effects of these compounds may be unrelated to the inhibition of the XO, the encouraging findings rekindled significant interest in the development of additional, novel series of XO inhibitors for various therapeutic indications. Here we present a critical overview of the effects of XO inhibitors in various pathophysiological conditions and also review the various emerging therapeutic strategies offered by this approach.
Figures
References
-
- Ahn SY, Sugi K, Talke P, Theissen JL, Linares HA, Traber LD, Herndon DN, Traber DL. Effects of allopurinol on smoke inhalation in the ovine model. J Appl Physiol. 1990;68:228–234. - PubMed
-
- Aiba M, Yokoyama Y, Snow TR, Novitzky D, McKeown PP. Effects of allopurinol pretreatment with pulmonary flush on lung preservation. J Heart Lung Transplant. 1992;11:1025–1030. - PubMed
-
- Akdemir H, Asik Z, Pasaoglu H, Karakucuk I, Oktem IS, Koc RK. The effect of allopurinol on focal cerebral ischaemia: an experimental study in rabbits. Neurosurg Rev. 2001;24:131–135. - PubMed
-
- Akizuki S, Yoshida S, Chambers DE, Eddy LJ, Parmley LF, Yellon DM, Downey JM. Infarct size limitation by the xanthine oxidase inhibitor, allopurinol, in closed-chest dogs with small infarcts. Cardiovasc Res. 1985;19:686–692. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
