

Severely impaired insulin signaling in chronic wounds of diabetic ob/ob mice: a potential role of tumor necrosis factor-alpha
- PMID: 16507892
- PMCID: PMC1606528
- DOI: 10.2353/ajpath.2006.050293
Severely impaired insulin signaling in chronic wounds of diabetic ob/ob mice: a potential role of tumor necrosis factor-alpha
Abstract
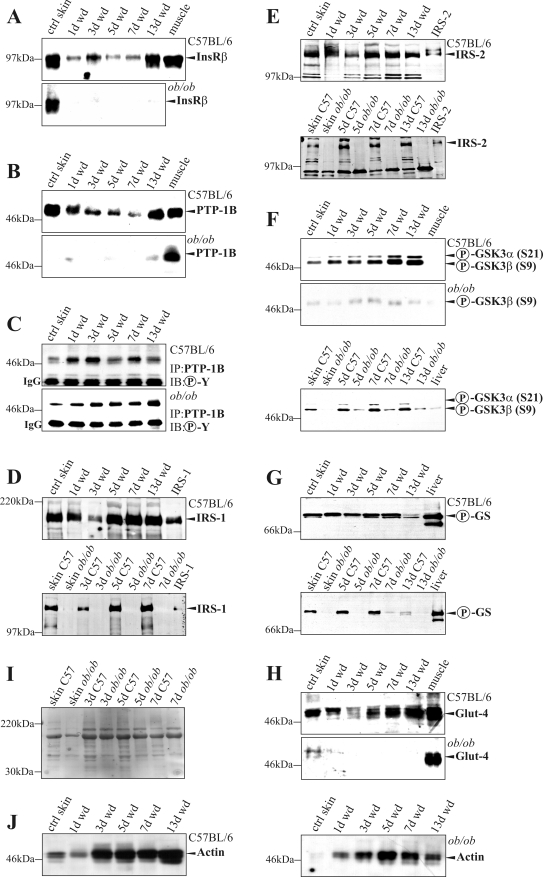
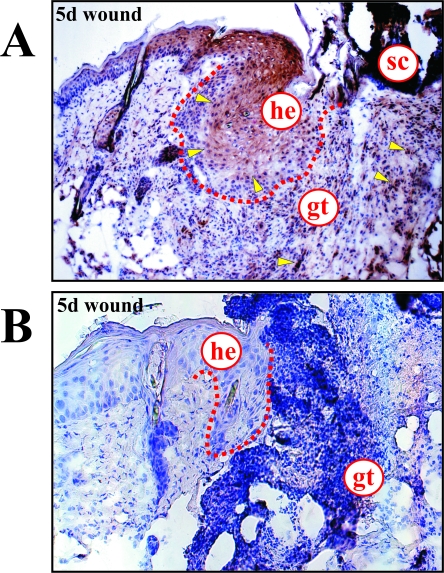
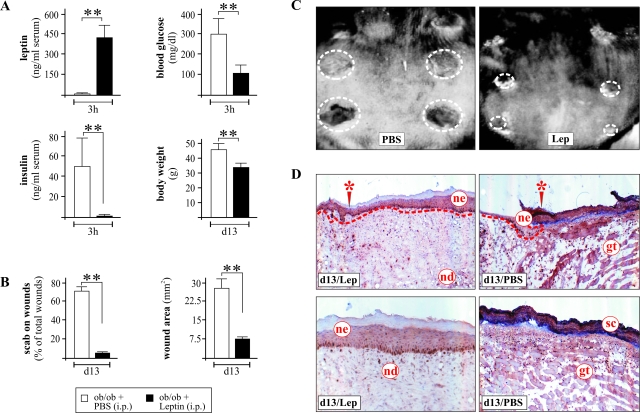
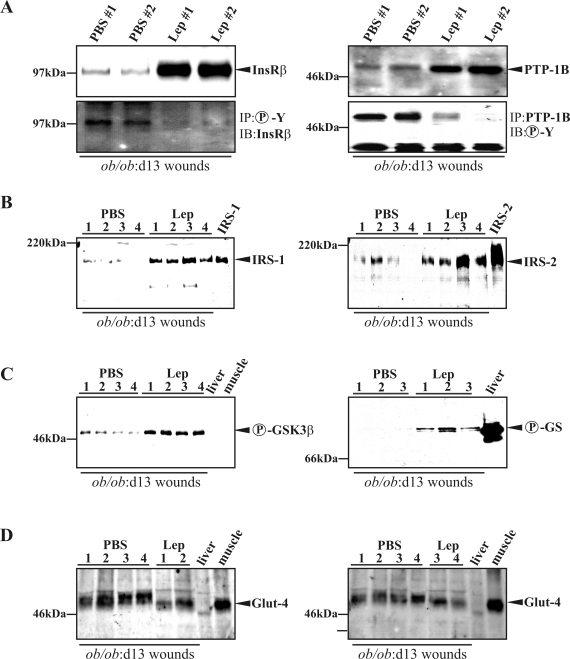
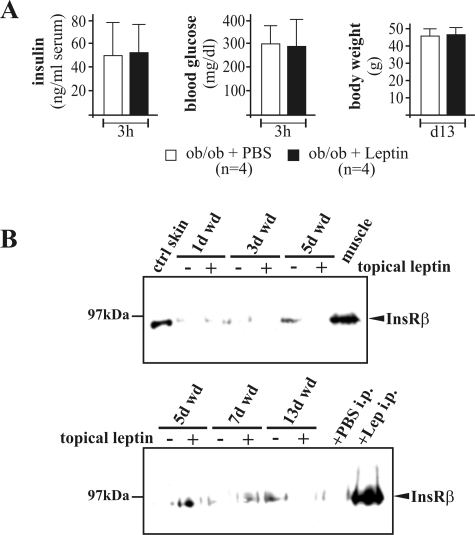
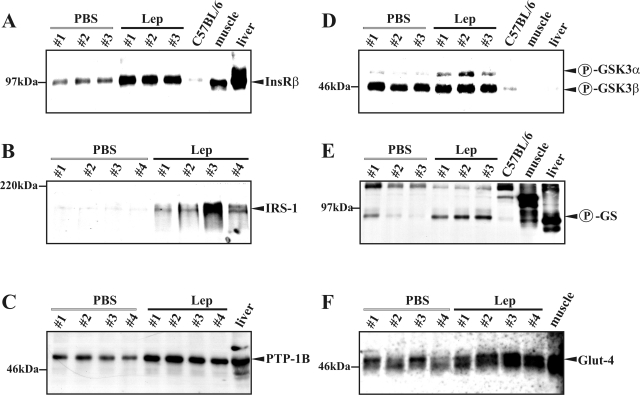
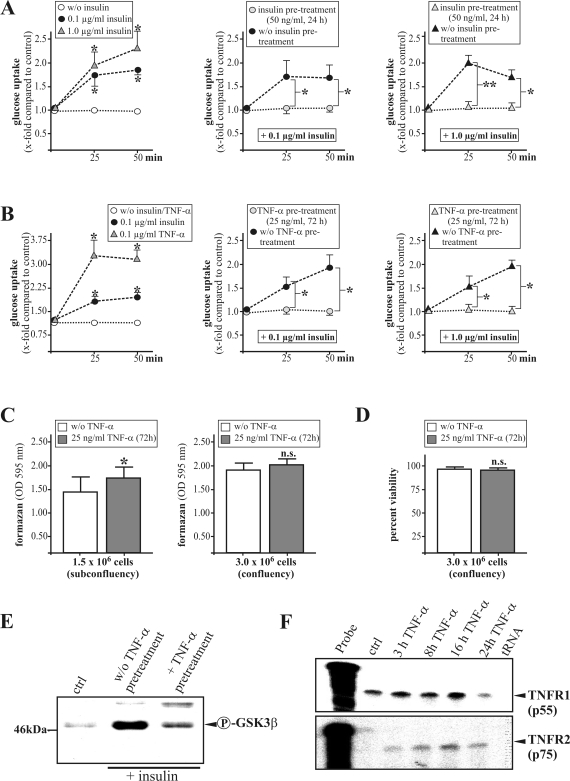
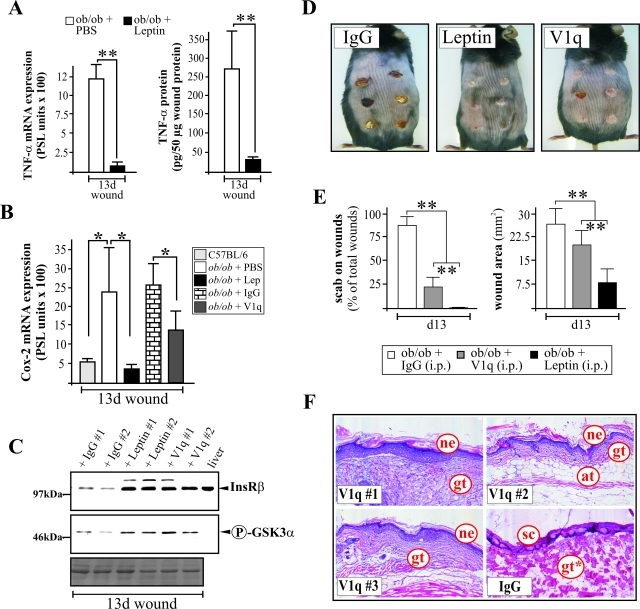
Wound-healing disorders are major complications of diabetes mellitus. Here, we investigated insulin-mediated signaling in nonwounded skin and in cutaneous tissue regeneration of healthy C57BL/6 and diabetes-impaired leptin-deficient obese/obese (ob/ob) mice. The insulin receptor (InsR) was abundantly expressed in wound margins and granulation tissue during acute healing in healthy mice. Remarkably, active signaling from the InsR, as assessed by phosphorylation of downstream targets such as protein tyrosine phosphatase-1B, glycogen synthase (GS), and GS kinase, was nearly absent in nonwounded and acutely healing skin from ob/ob mice. Systemic leptin administration to ob/ob mice reverted the diabetic phenotype and improved tissue regeneration as well as the impaired expression of InsR, insulin receptor substrate-1 and insulin receptor substrate-2, and downstream signaling (phosphorylation of GS kinase and GS) in late wounds and nonwounded skin of ob/ob mice. Importantly, tumor necrosis factor (TNF)-alpha was a mediator of insulin resistance in keratinocytes in vitro and in ob/ob wound tissue in vivo. Systemic administration of a monoclonal anti-TNF-alpha antibody (V1q) in wounded ob/ob mice attenuated wound inflammation, improved re-epithelialization, and restored InsR expression and signaling in wound tissue of ob/ob mice. These data suggest that InsR signaling in diabetes-impaired wounds is sensitive to inflammatory conditions and that anti-inflammatory approaches, such as anti-TNF-alpha strategies, improve diabetic wound healing.
Figures

Similar articles
-
Systemic anti-TNFalpha treatment restores diabetes-impaired skin repair in ob/ob mice by inactivation of macrophages.J Invest Dermatol. 2007 Sep;127(9):2259-67. doi: 10.1038/sj.jid.5700842. Epub 2007 Apr 26. J Invest Dermatol. 2007. PMID: 17460730
-
Systemically and topically supplemented leptin fails to reconstitute a normal angiogenic response during skin repair in diabetic ob/ob mice.Diabetologia. 2001 Apr;44(4):471-9. doi: 10.1007/s001250051645. Diabetologia. 2001. PMID: 11357478
-
Leptin enhances wound re-epithelialization and constitutes a direct function of leptin in skin repair.J Clin Invest. 2000 Aug;106(4):501-9. doi: 10.1172/JCI9148. J Clin Invest. 2000. PMID: 10953025 Free PMC article.
-
Metabolism and insulin signaling in common metabolic disorders and inherited insulin resistance.Dan Med J. 2014 Jul;61(7):B4890. Dan Med J. 2014. PMID: 25123125 Review.
-
Insulin resistance induced by tumor necrosis factor-alpha in myocytes and brown adipocytes.J Anim Sci. 2008 Apr;86(14 Suppl):E94-104. doi: 10.2527/jas.2007-0462. Epub 2007 Oct 16. J Anim Sci. 2008. PMID: 17940160 Review.
Cited by
-
Wound healing in mice with high-fat diet- or ob gene-induced diabetes-obesity syndromes: a comparative study.Exp Diabetes Res. 2010;2010:476969. doi: 10.1155/2010/476969. Epub 2011 Jan 20. Exp Diabetes Res. 2010. PMID: 21318183 Free PMC article.
-
Effect of novel blend nanofibrous scaffolds on diabetic wounds healing.IET Nanobiotechnol. 2016 Feb;10(1):1-7. doi: 10.1049/iet-nbt.2014.0066. IET Nanobiotechnol. 2016. PMID: 26766866 Free PMC article.
-
Expression of PKM2 in wound keratinocytes is coupled to angiogenesis during skin repair in vivo and in HaCaT keratinocytes in vitro.J Mol Med (Berl). 2023 Feb;101(1-2):151-169. doi: 10.1007/s00109-022-02280-6. Epub 2023 Jan 12. J Mol Med (Berl). 2023. PMID: 36633604 Free PMC article.
-
Sleep fragmentation delays wound healing in a mouse model of type 2 diabetes.Sleep. 2018 Nov 1;41(11):zsy156. doi: 10.1093/sleep/zsy156. Sleep. 2018. PMID: 30107617 Free PMC article.
-
A transgenic mouse model of inducible macrophage depletion: effects of diphtheria toxin-driven lysozyme M-specific cell lineage ablation on wound inflammatory, angiogenic, and contractive processes.Am J Pathol. 2009 Jul;175(1):132-47. doi: 10.2353/ajpath.2009.081002. Epub 2009 Jun 15. Am J Pathol. 2009. PMID: 19528348 Free PMC article.
References
-
- Pryce TD. A case of perforating ulcers of both feet associated with diabetes and ataxic symptoms. Lancet. 1887;2:11–12.
-
- Boulton AJM. The diabetic foot: from art to science. The 18th Camillo Golgi lecture. Diabetologia. 2004;47:1343–1353. - PubMed
-
- Reiber GE, Ledoux WR. Epidemiology of diabetic foot ulcers and amputations: evidence for prevention. Williams R, Herman W, AL Kinmonth, Wareham NJ, editors. Chichester: UK, Wiley; The Evidence Base for Diabetes Care. 2002:pp 641–665.
-
- Carrington AL, Abbott CA, Griffiths J, Jackson N, van Ross ERE, Boulton AJM. A foot care program for diabetic unilateral amputees. Diabetes Care. 2001;24:216–221. - PubMed
-
- Abbott CA, Carrington AL, Ashe H, Bath S, Every LC, Griffiths J, Hann AW, Hussein A, Jackson N, Johnson KE, Ryder CH, Torkington R, Van Ross ER, Whalley AM, Widdows P, Williamson S, Boulton AJ. The North-West Diabetes Foot Care Study: incidence of, and risk factors for, new diabetic foot ulceration in a community-based patient cohort. Diabetic Med. 2002;20:377–384. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
