

The effect of methodological differences in the measurement of stapes motion in live and cadaver ears
- PMID: 16514236
- PMCID: PMC2917778
- DOI: 10.1159/000091815
The effect of methodological differences in the measurement of stapes motion in live and cadaver ears
Abstract
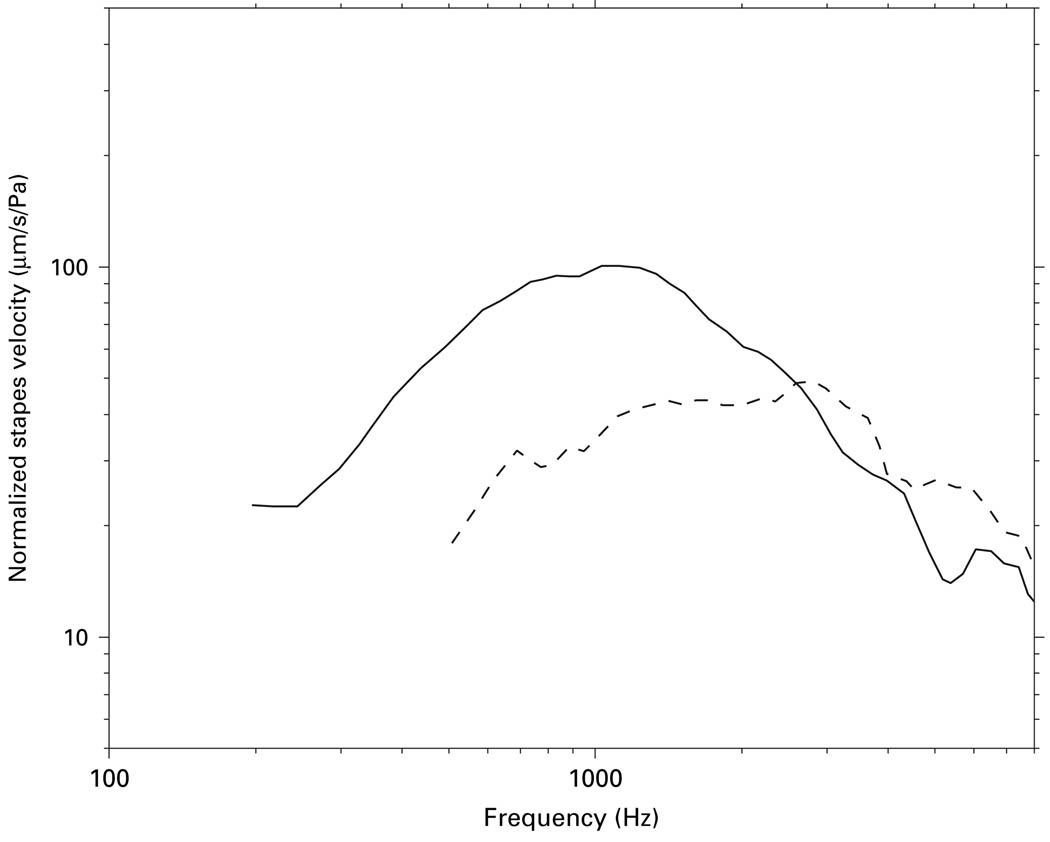
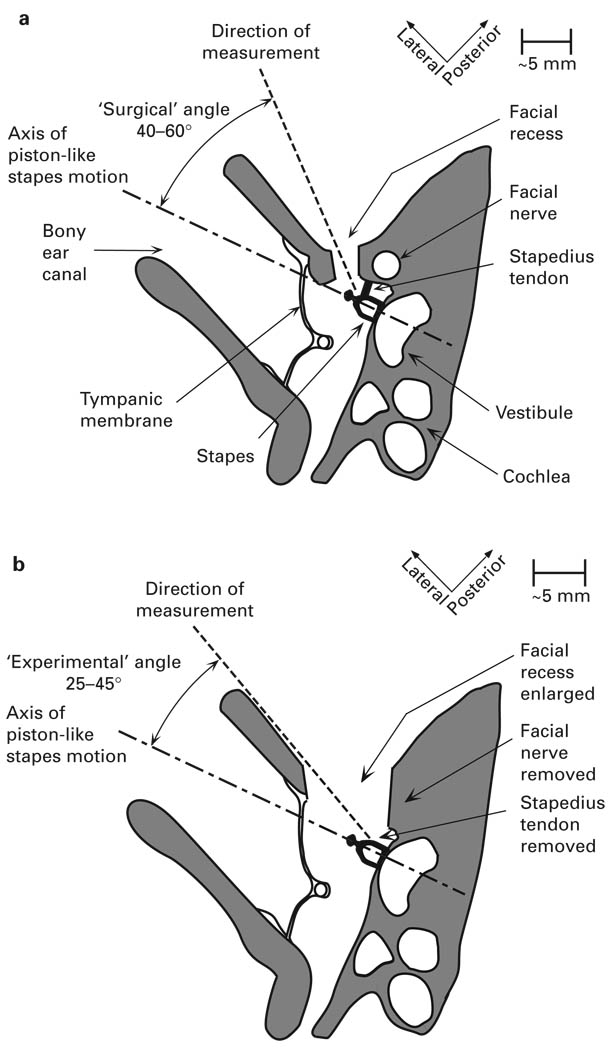
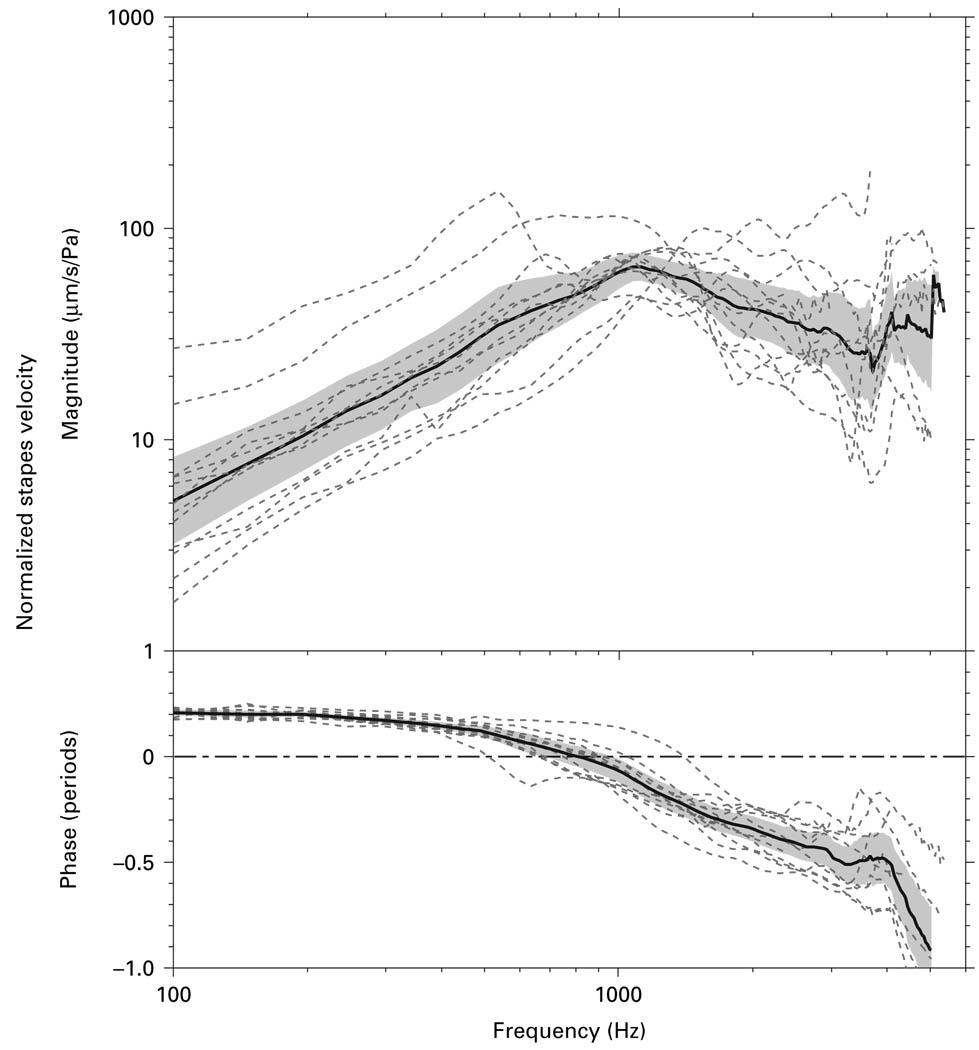
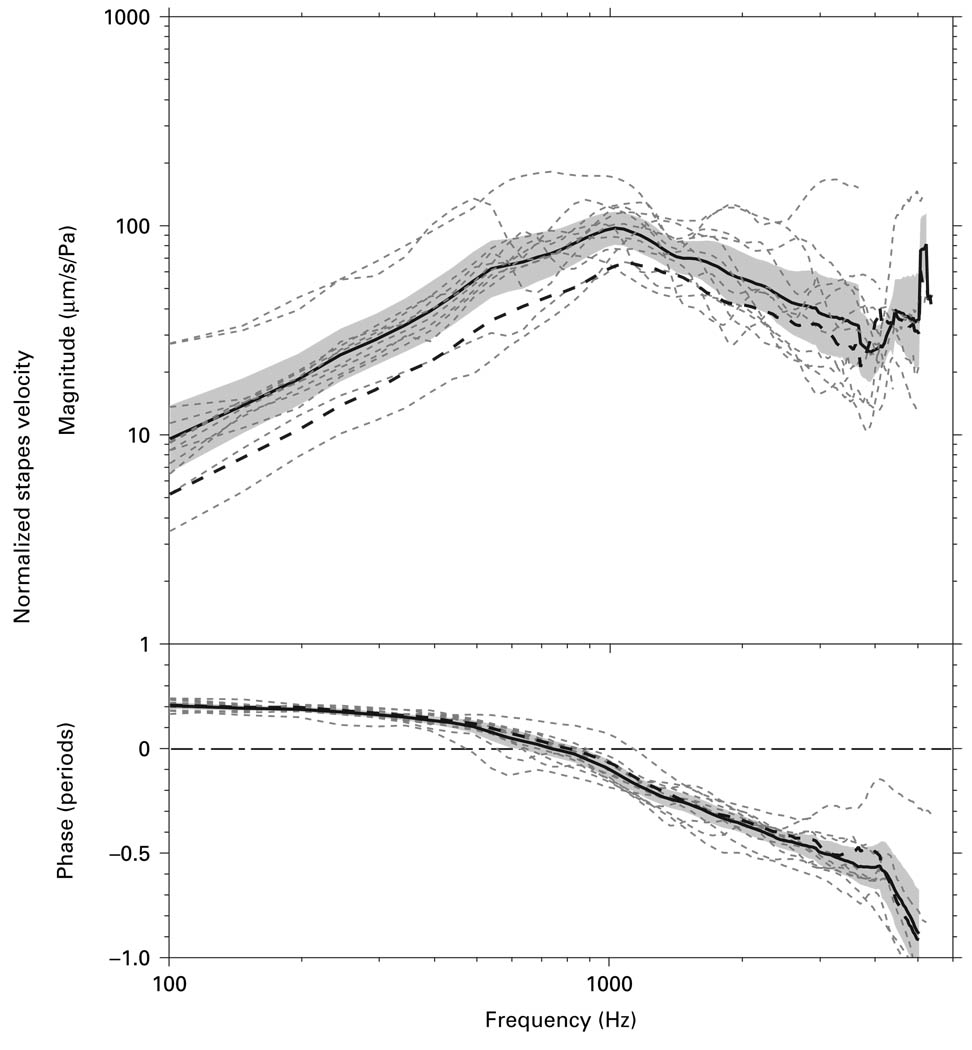
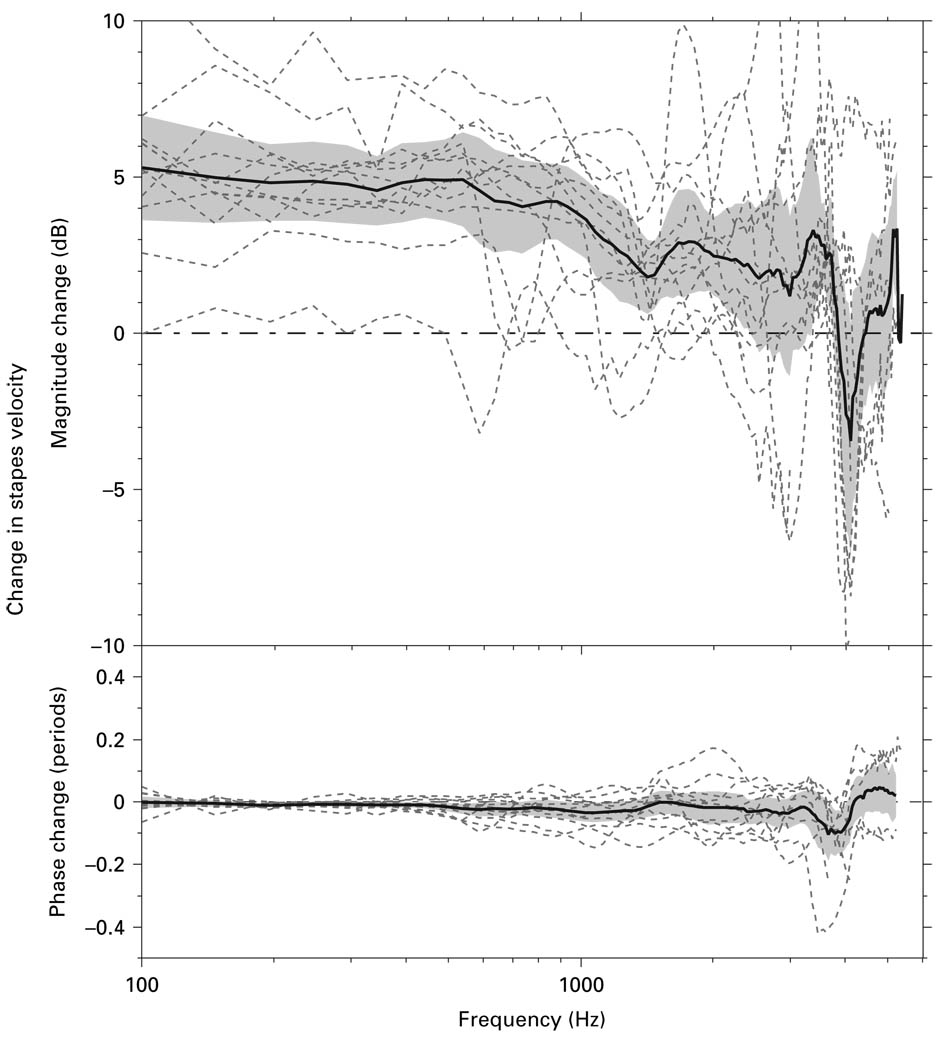
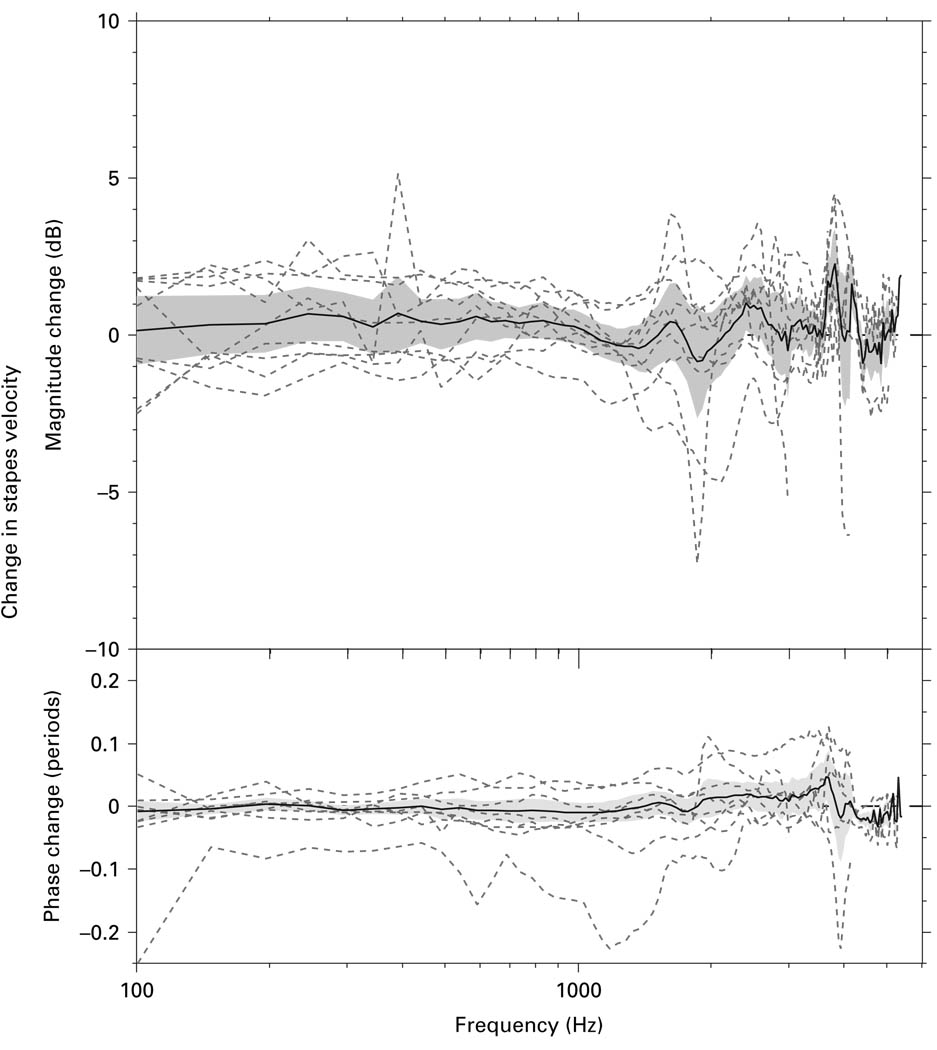
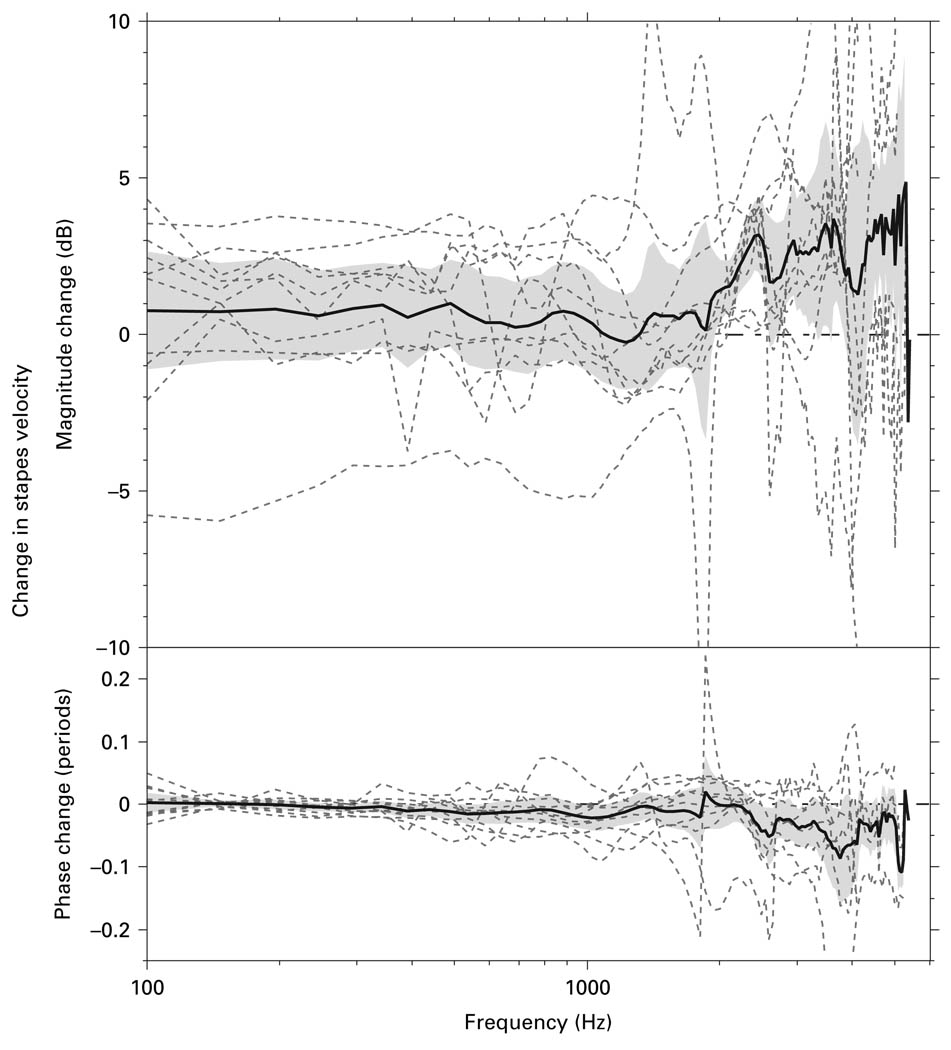
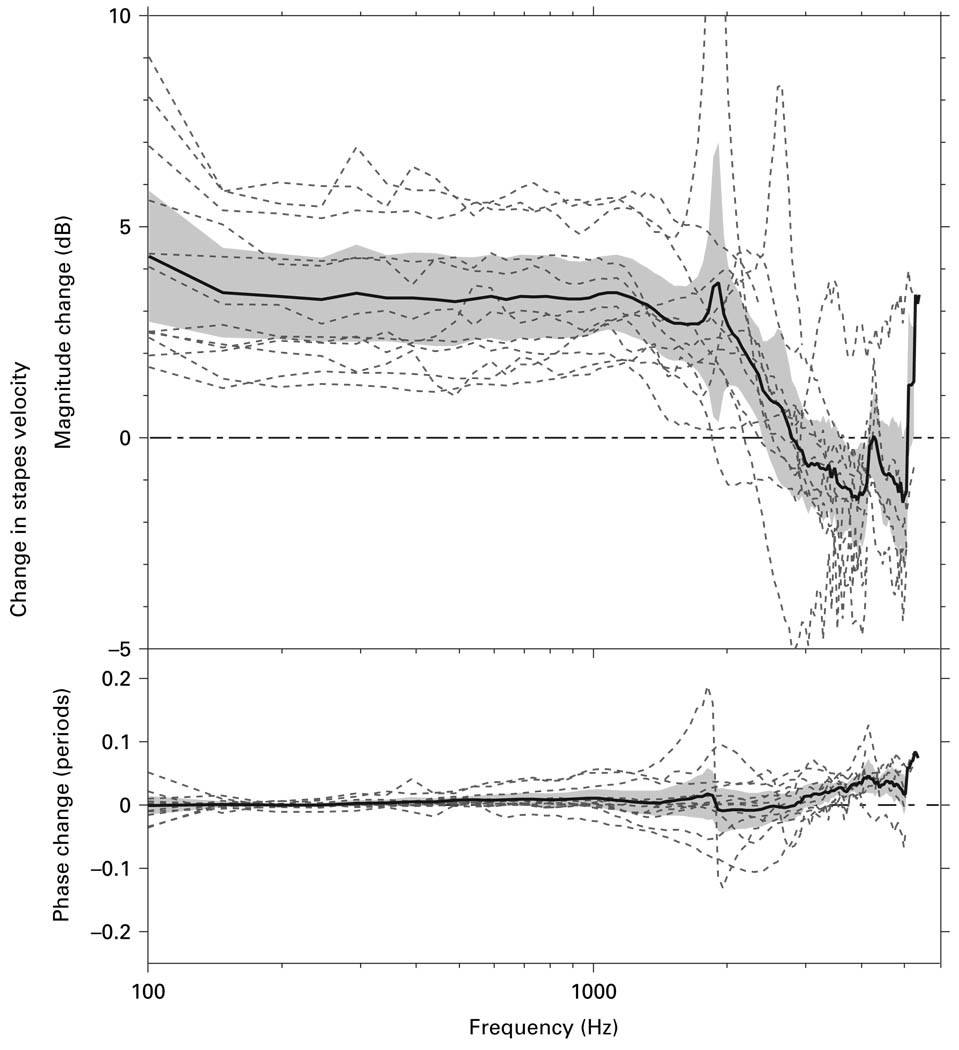
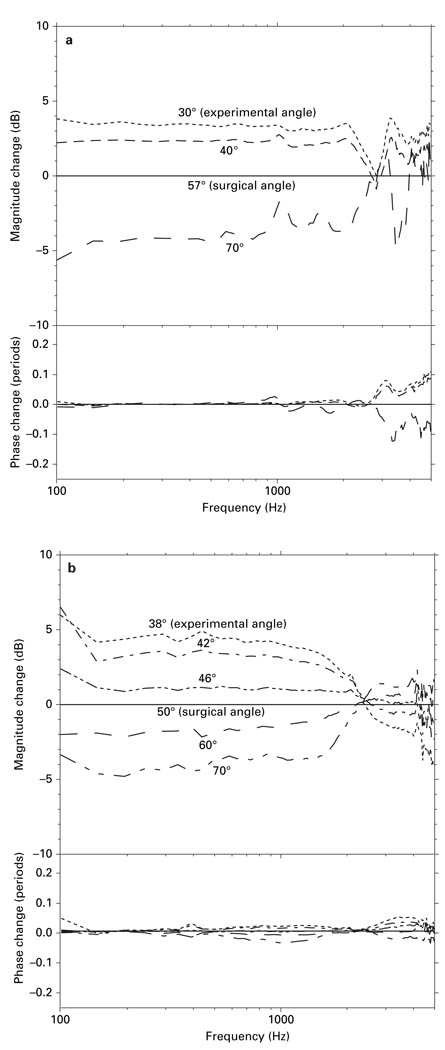
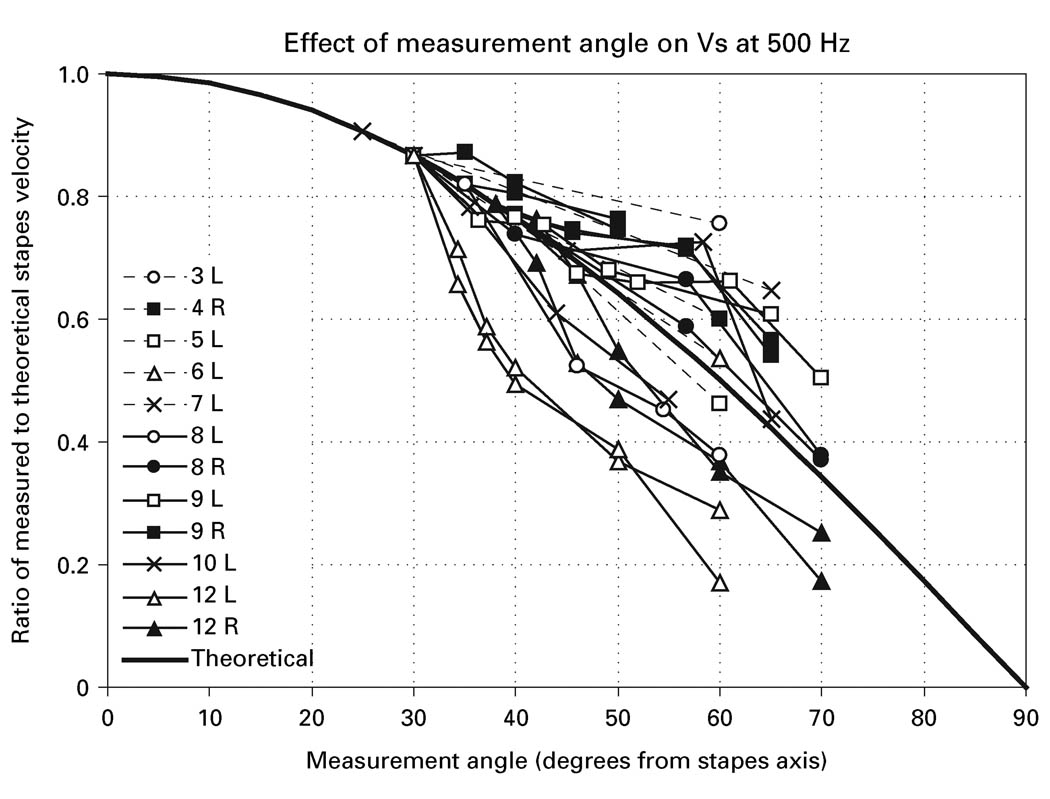
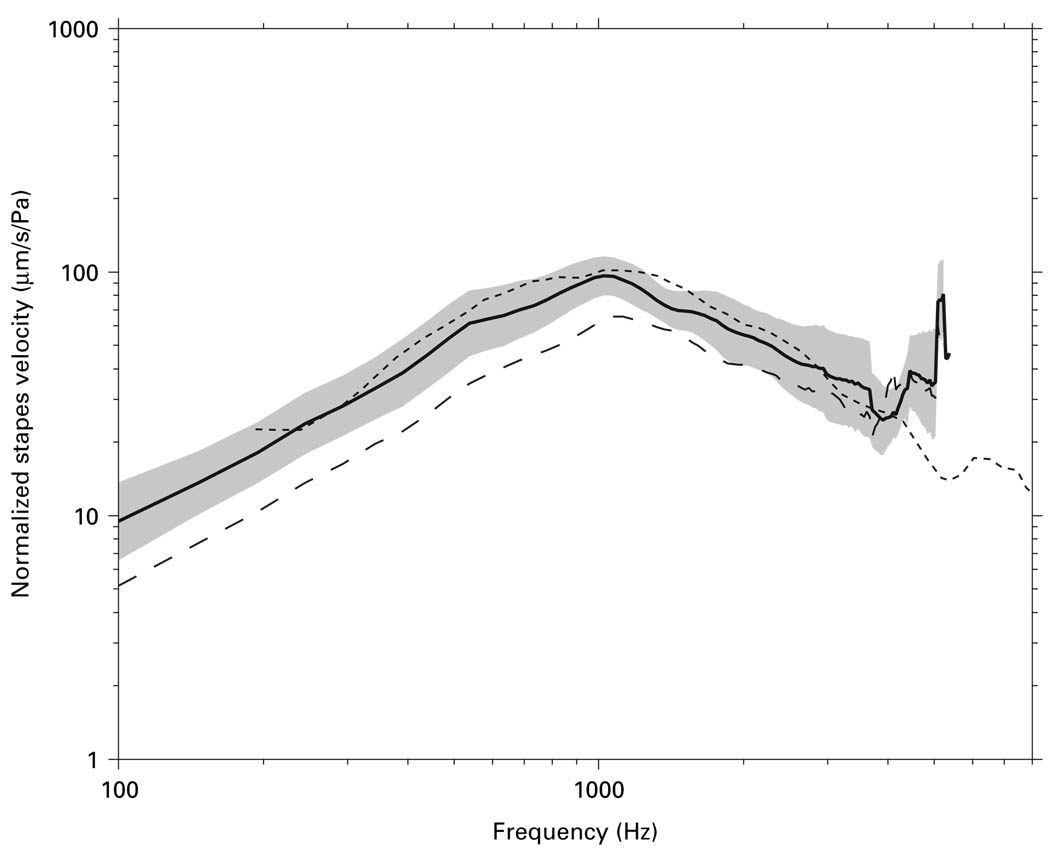
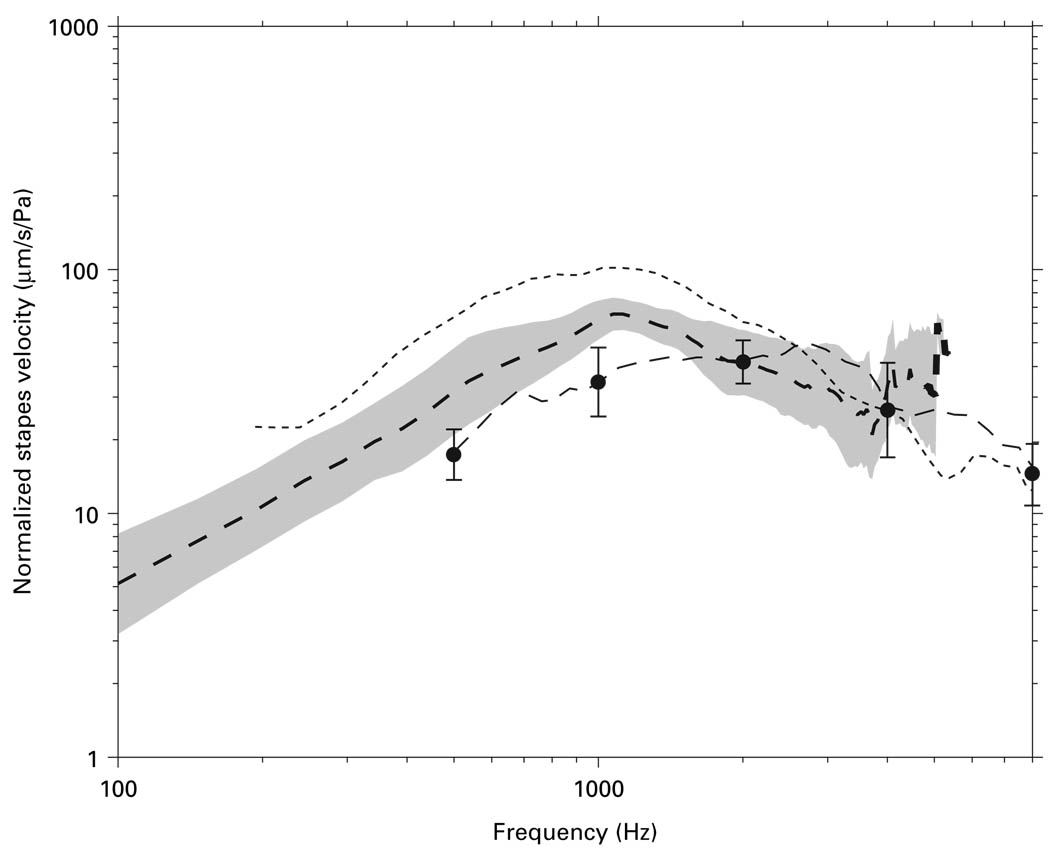
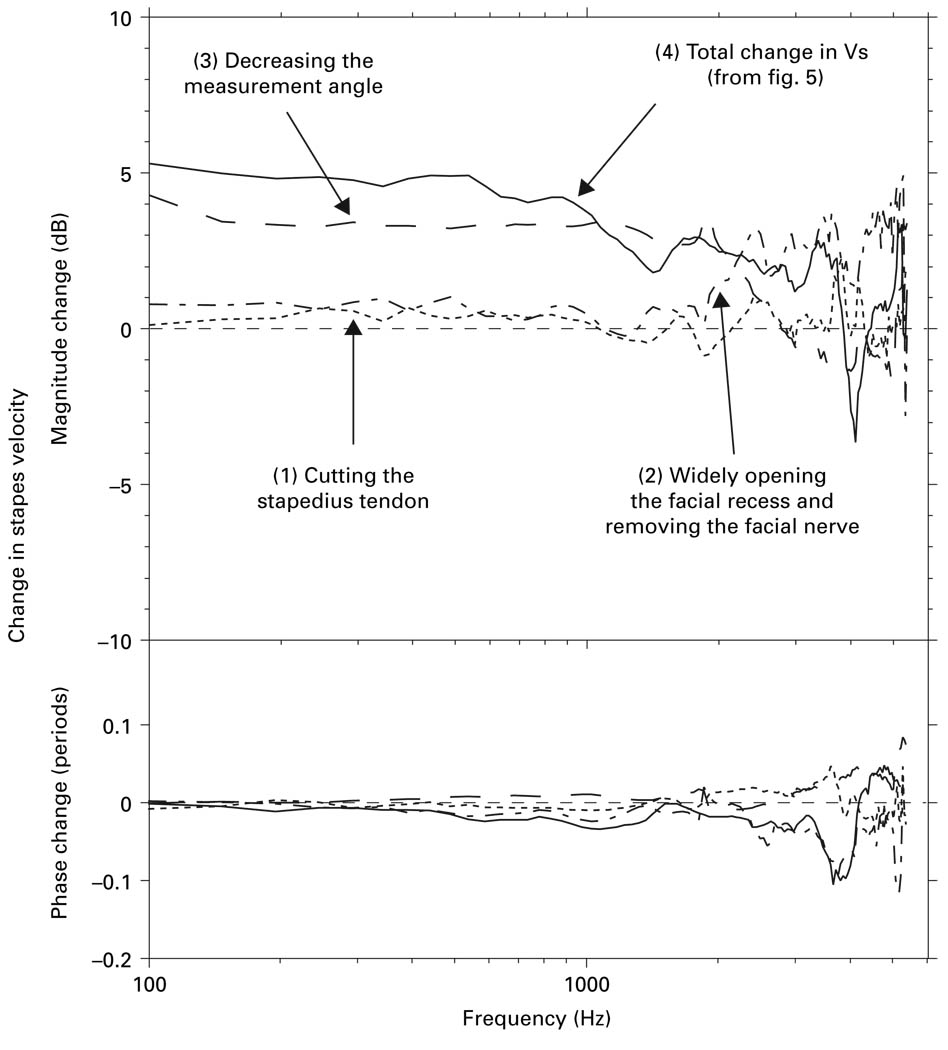
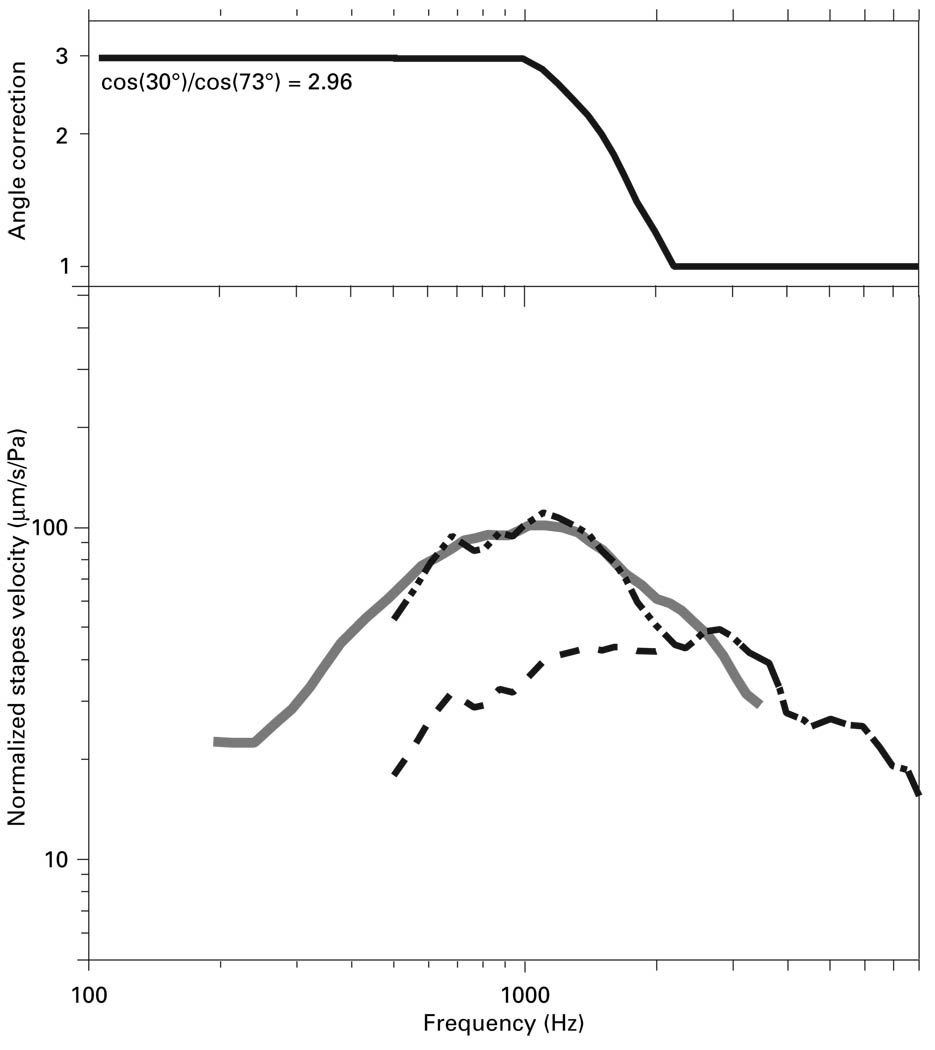
Methodological differences in sound-induced stapes velocity (Vs) measurements in live and cadaveric ears were examined using fresh cadaveric temporal bones. On average, differences in preparation (sectioning the stapedius tendon, removing the facial nerve, and widely opening the facial recess) had statistically insignificant effects on measured Vs. Differences in the achievable measurement angle (with respect to the axis of piston-like stapes motion) had a significant effect on measured Vs below 2 kHz. These results suggest that much if not all of the differences in Vs measurements between live and cadaveric ears can be explained by the differences in measurement angle between the two preparations. Measurement angle was found to have minimal effect on measured Vs above 2 kHz. This demonstrates that the commonly used method of estimating stapes translational velocity by dividing the measured velocity by the cosine of the measurement angle is not valid above 2 kHz.
Copyright (c) 2006 S. Karger AG, Basel.
Figures
References
-
- Asai M, Huber A, Goode R. Analysis of the best site on the stapes footplate for ossicular chain reconstruction. Acta Otolaryngol (Stockh) 1999;119:356–361. - PubMed
-
- Decraemer WF, Khanna SM. Measurement, visualization and quantitative analysis of complete three-dimensional kinematical data sets of human and cat middle ear. In: Gyo K, Wada H, Hato N, Koike T, editors. Middle Ear Mechanics in Research and Otology. Singapore: World Scientific; 2004. pp. 3–10.
-
- Goode RL, Ball G, Nishihara S. Measurement of umbo vibration in human subjects – method and possible clinical applications. Am J Otol. 1993;14:247–251. - PubMed
-
- Goode RL, Ball G, Nishihara S, Nakamura K. Laser Doppler vibrometer (LDV) – a new clinical tool for the otologist. Am J Otol. 1996;17:813–822. - PubMed
-
- Gyo K, Aritomo H, Goode RL. Measurement of the ossicular vibration ratio in human temporal bones by use of a video measuring system. Acta Otolaryngol. 1987;103:87–95. - PubMed
