

Hypnosis Antenatal Training for Childbirth (HATCh): a randomised controlled trial [NCT00282204]
- PMID: 16515709
- PMCID: PMC1450315
- DOI: 10.1186/1471-2393-6-5
Hypnosis Antenatal Training for Childbirth (HATCh): a randomised controlled trial [NCT00282204]
Abstract
Background: Although medical interventions play an important role in preserving lives and maternal comfort they have become increasingly routine in normal childbirth. This may increase the risk of associated complications and a less satisfactory birth experience. Antenatal hypnosis is associated with a reduced need for pharmacological interventions during childbirth. This trial seeks to determine the efficacy or otherwise of antenatal group hypnosis preparation for childbirth in late pregnancy.
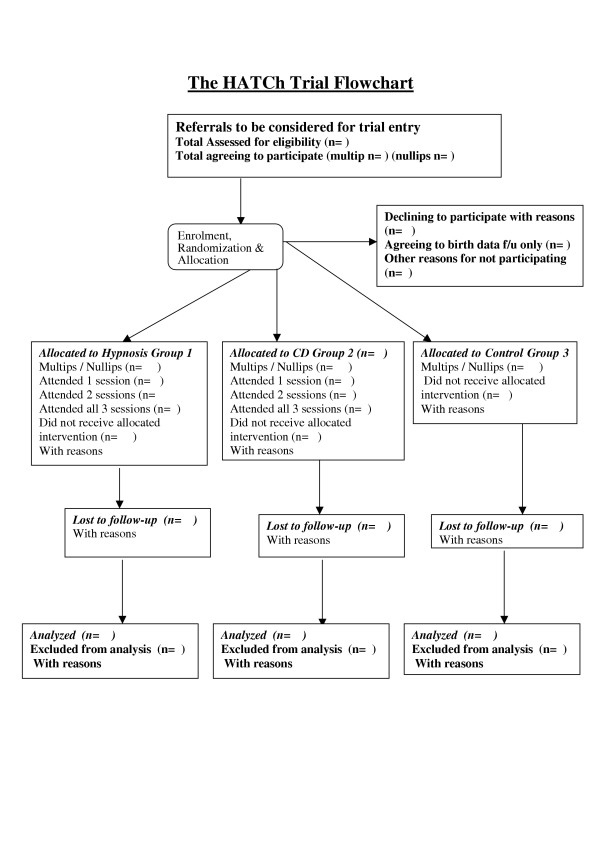
Methods/design: A single centre, randomised controlled trial using a 3 arm parallel group design in the largest tertiary maternity unit in South Australia. Group 1 participants receive antenatal hypnosis training in preparation for childbirth administered by a qualified hypnotherapist with the use of an audio compact disc on hypnosis for re-enforcement; Group 2 consists of antenatal hypnosis training in preparation for childbirth using an audio compact disc on hypnosis administered by a nurse with no training in hypnotherapy; Group 3 participants continue with their usual preparation for childbirth with no additional intervention. Women > 34 and < 39 weeks gestation, planning a vaginal birth, not in active labour, with a singleton, viable fetus of vertex presentation, are eligible to participate. Allocation concealment is achieved using telephone randomisation. Participants assigned to hypnosis groups commence hypnosis training as near as possible to 37 weeks gestation. Treatment allocations are concealed from treating obstetricians, anaesthetists, midwives and those personnel collecting and analysing data. Our sample size of 135 women/group gives the study 80% power to detect a clinically relevant fall of 20% in the number of women requiring pharmacological analgesia - the primary endpoint. We estimate that approximately 5-10% of women will deliver prior to receiving their allocated intervention. We plan to recruit 150 women/group and perform sequential interim analyses when 150 and 300 participants have been recruited. All participant data will be analysed, by a researcher blinded to treatment allocation, according to the "Intention to treat" principle with comprehensive pre-planned cost- benefit and subgroup analyses.
Discussion: If effective, hypnosis would be a simple, inexpensive way to improve the childbirth experience, reduce complications associated with pharmacological interventions, yield cost savings in maternity care, and this trial will provide evidence to guide clinical practice.
References
-
- ANZCA working party . The pregnant patient. In: Macintyre P, editor. Acute pain management: Scientific evidence. 2. Melbourne: Australian and New Zealand College of Anaesthetists and the Faculty of Pain Medicine; 2005. pp. 222–237.
-
- Bromage PR. Neurologic Complications of Labor, Delivery, and Regional Anesthesia. In: Chestnut DH, editor. Obstetric anesthesia. St. Louis: Mosby; 1999. pp. 639–61.
-
- Weeks S. Postpartum Headache. In: Chestnut DH, editor. Obstetric anaesthesia. St. Louis: Mosby; 1999. pp. 621–38.
LinkOut - more resources
Full Text Sources
Medical
