

Modelling the impact of antiretroviral use in resource-poor settings
- PMID: 16519553
- PMCID: PMC1395349
- DOI: 10.1371/journal.pmed.0030124
Modelling the impact of antiretroviral use in resource-poor settings
Abstract
Background: The anticipated scale-up of antiretroviral therapy (ART) in high-prevalence, resource-constrained settings requires operational research to guide policy on the design of treatment programmes. Mathematical models can explore the potential impacts of various treatment strategies, including timing of treatment initiation and provision of laboratory monitoring facilities, to complement evidence from pilot programmes.
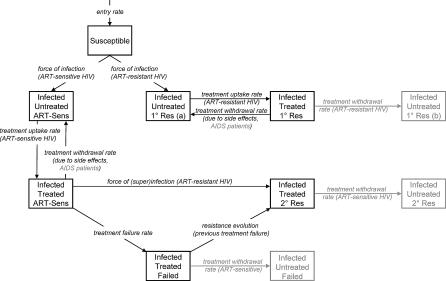
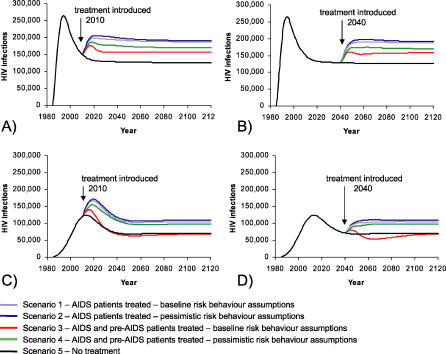
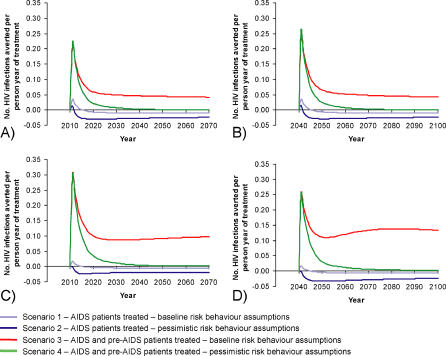
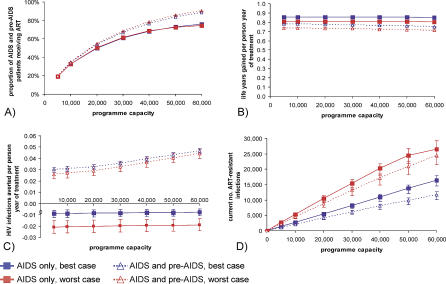
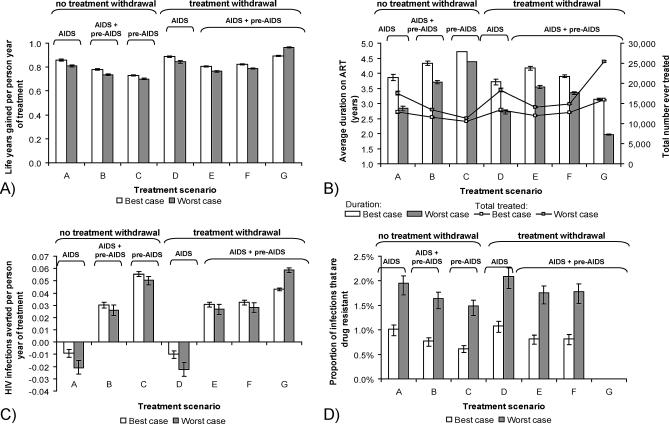
Methods and findings: A deterministic model of HIV transmission incorporating ART and stratifying infection progression into stages was constructed. The impact of ART was evaluated for various scenarios and treatment strategies, with different levels of coverage, patient eligibility, and other parameter values. These strategies included the provision of laboratory facilities that perform CD4 counts and viral load testing, and the timing of the stage of infection at which treatment is initiated. In our analysis, unlimited ART provision initiated at late-stage infection (AIDS) increased prevalence of HIV infection. The effect of additionally treating pre-AIDS patients depended on the behaviour change of treated patients. Different coverage levels for ART do not affect benefits such as life-years gained per person-year of treatment and have minimal effect on infections averted when treating AIDS patients only. Scaling up treatment of pre-AIDS patients resulted in more infections being averted per person-year of treatment, but the absolute number of infections averted remained small. As coverage increased in the models, the emergence and risk of spread of drug resistance increased. Withdrawal of failing treatment (clinical resurgence of symptoms), immunologic (CD4 count decline), or virologic failure (viral rebound) increased the number of infected individuals who could benefit from ART, but effectiveness per person is compromised. Only withdrawal at a very early stage of treatment failure, soon after viral rebound, would have a substantial impact on emergence of drug resistance.
Conclusions: Our analysis found that ART cannot be seen as a direct transmission prevention measure, regardless of the degree of coverage. Counselling of patients to promote safe sexual practices is essential and must aim to effect long-term change. The chief aims of an ART programme, such as maximised number of patients treated or optimised treatment per patient, will determine which treatment strategy is most effective.
Conflict of interest statement
Figures
Comment in
-
Modeling the impact of antiretroviral use in developing countries.PLoS Med. 2006 Apr;3(4):e148. doi: 10.1371/journal.pmed.0030148. Epub 2006 Mar 14. PLoS Med. 2006. PMID: 16522134 Free PMC article.
References
-
- Palella F, Delaney K, Moorman A, Loveless M, Fuhrer J, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. N Engl J Med. 1998;338:853–860. - PubMed
-
- Quinn TC, Wawer MJ, Sewankambo N, Serwadda D, Li C, et al. Viral load and heterosexual transmission of human immunodeficiency virus type 1. Rakai Project Study Group. N Engl J Med. 2000;342:921–929. - PubMed
-
- Velasco-Hernandez J, Gershengorn H, Blower S. Could widespread use of combination antiretroviral therapy eradicate HIV epidemics? Lancet Infect Dis. 2002;2:487–493. - PubMed
-
- Boily MC, Lowndes CM, Alary M. Complementary hypothesis concerning the community sexually transmitted disease mass treatment puzzle in Rakai, Uganda. AIDS. 2000;14:2583–2592. - PubMed
-
- Hearst N, Chen S. Condom promotion for AIDS prevention in the developing world: Is it working? Stud Fam Plann. 2004;35:39–47. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
