

Cyclooxygenase-2 and epithelial growth factor receptor up-regulation during progression of Barrett's esophagus to adenocarcinoma
- PMID: 16521222
- PMCID: PMC4066159
- DOI: 10.3748/wjg.v12.i6.928
Cyclooxygenase-2 and epithelial growth factor receptor up-regulation during progression of Barrett's esophagus to adenocarcinoma
Abstract
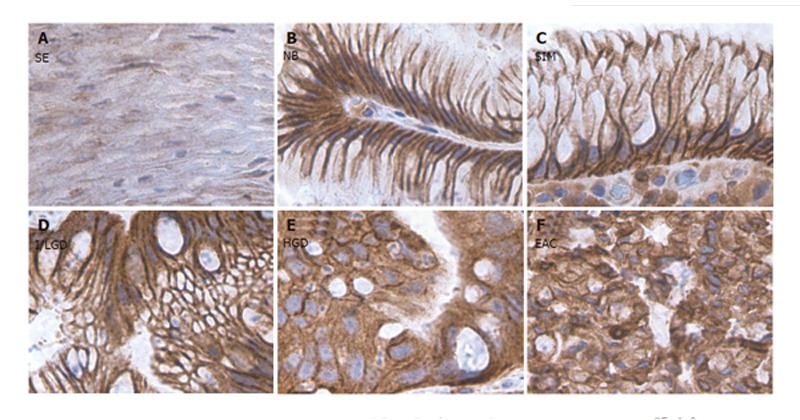
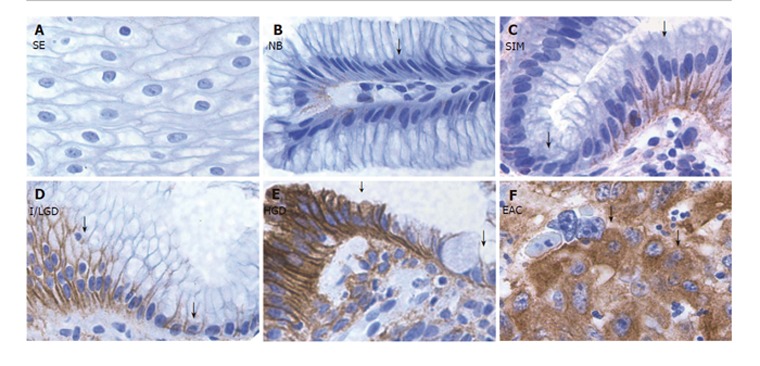
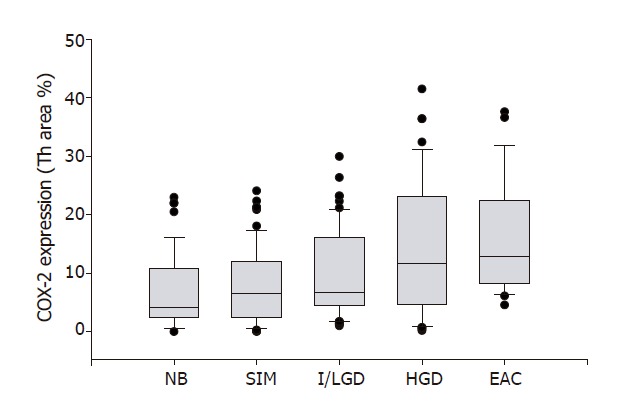
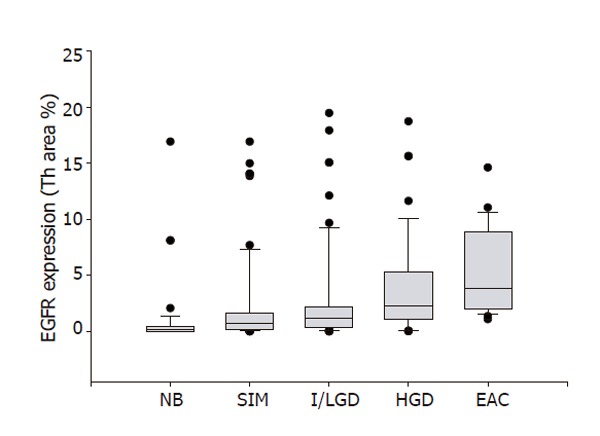
Aim: To investigate the expression of cyclooxygenase-2 (COX-2) and epithelial growth factor receptor (EGFR) throughout the progression of Barretts esophagus (BE).
Methods: COX-2 and EGFR protein expressions were detected by using immunohistochemical method. A detailed cytomorphological changes were determined. Areas of COX-2 and EGFR expression were quantified by using computer Imaging System.
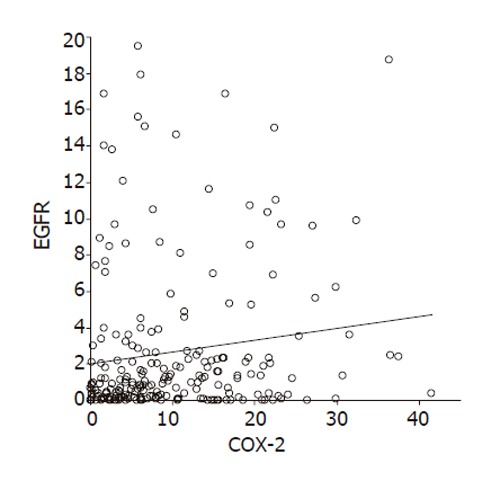
Results: The expressions of both COX-2 and EGFR increased along with the progression from BE to esophagus adenocarcinoma (EAC). A positive correlation was found between COX-2 expression and EGFR expression.
Conclusion: COX-2 and EGFR may be cooperative in the stepwise progression from BE to EAC, thereby leading to carcinogenesis.
Figures
References
-
- Blot WJ, Devesa SS, Kneller RW, Fraumeni JF Jr. Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA. 1991;265:1287–1289. - PubMed
-
- Pera M, Cameron AJ, Trastek VF, Carpenter HA, Zinsmeister AR. Increasing incidence of adenocarcinoma of the esophagus and esophagogastric junction. Gastroenterology. 1993;104:510–513. - PubMed
-
- Farrow DC, Vaughan TL. Determinants of survival following the diagnosis of esophageal adenocarcinoma (United States) Cancer Causes Control. 1996;7:322–327. - PubMed
-
- Isolauri J, Luostarinen M, Isolauri E, Reinikainen P, Viljakka M, Keyriläinen O. Natural course of gastroesophageal reflux disease: 17-22 year follow-up of 60 patients. Am J Gastroenterol. 1997;92:37–41. - PubMed
-
- Altorki NK, Oliveria S, Schrump DS. Epidemiology and molecular biology of Barrett's adenocarcinoma. Semin Surg Oncol. 1997;13:270–280. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
