

Cervical spine abnormalities associated with Down syndrome
- PMID: 16525818
- PMCID: PMC2532127
- DOI: 10.1007/s00264-005-0070-y
Cervical spine abnormalities associated with Down syndrome
Abstract
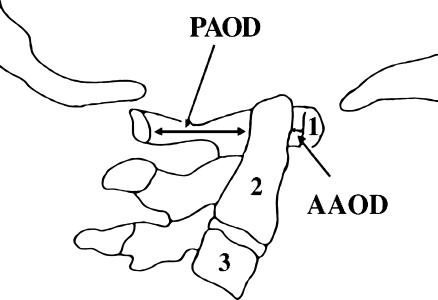
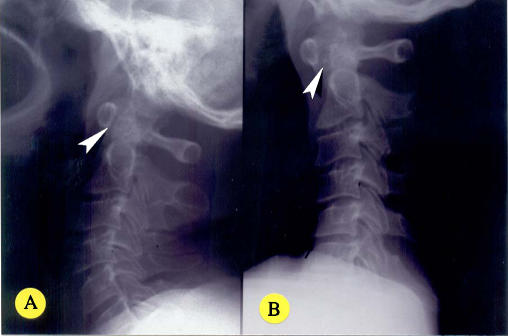
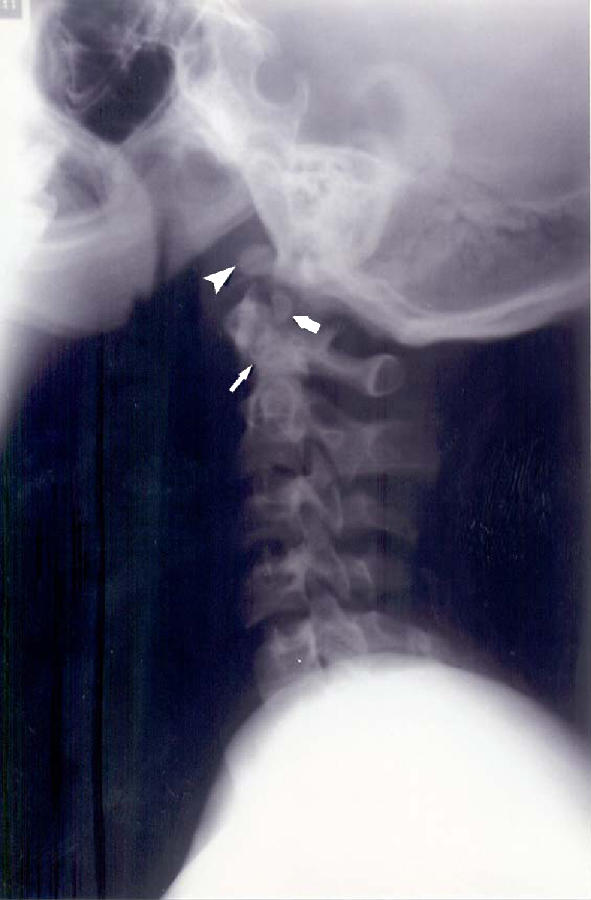
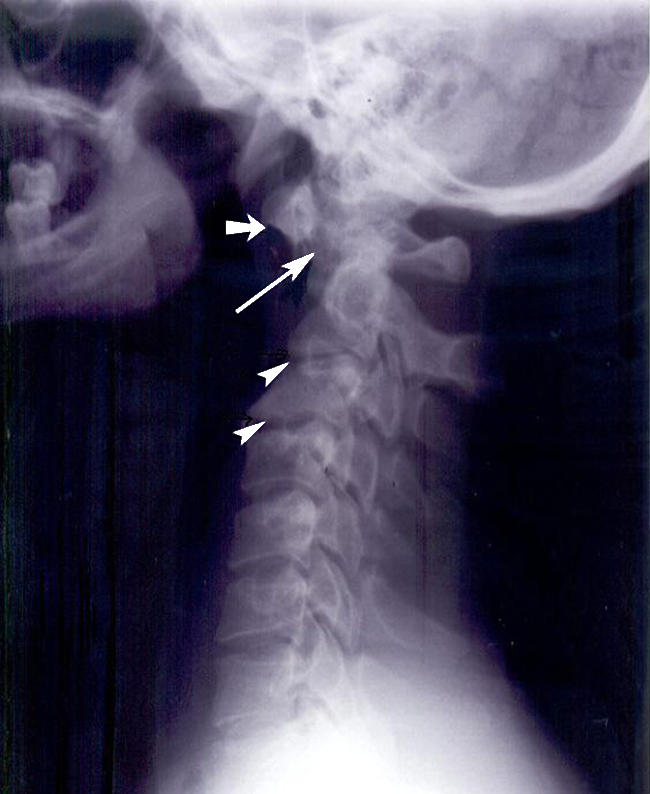
Atlantoaxial instability (AAI) affects 10-20% of individuals with Down syndrome (DS). The condition is mostly asymptomatic and diagnosed on radiography by an enlarged anterior atlanto-odontoid distance. Symptomatic AAI, which affects 1-2% of individuals with DS, manifests with spinal cord compression. Cervical spondylosis, which is common in DS, also has the potential for cord damage but it has received less attention because paediatric populations were mostly studied. Forty-four Kuwaiti subjects with DS, whose ages were > or = 15 years, were evaluated clinically and radiographically. Lateral neck radiographs were taken in the neutral and flexion positions. Asymptomatic AAI was diagnosed in eight subjects (18%) and congenital anomalies of C1-2 were found in five (12%). Five patients had AAI in flexion only while three patients had it in both views. Three patients with AAI had odontoid anomalies contributing to the condition. When assessing AAI, the posterior atlanto-odontoid distance has to be considered because it indicates the space available for the cord. Cervical spondylosis was noted in 16 (36%) subjects. Degenerative changes increased with age, occurred earlier than in the normal population, and affected mostly the lower cervical levels. Half the patients with AAI had cervical spondylosis, a comorbidity that puts the cord at increased risk.
L’instabilité de la charnière occipito atloïdienne affecte 10 à 20% des sujets présentant un Down syndrome (trisomie 21). Cette instabilité est souvent asymptomatique et seulement diagnostiquée sur les radiographies qui montrent un élargissement de la distance antérieure atloïdo-odontoide. L’asymptologie de l’instabilité occipito atloïdienne affecte 1 à 2% des sujets présentant un Down syndrome avec des signes manifestes de compression médullaire. La spondylose cervicale qui est habituelle dans le Down syndrome peut potentialiser des lésions de la moelle. 44 sujets Koweitis présentant un Down syndrome dont l’âge était supérieur à 15 ans ont été évalués cliniquement et radiographiquement. Des radiographies de la colonne cervicale de profil ont été effectuées en position neutre et en position de flexion. Une instabilité occipito atloïdienne a été diagnostiquée chez 8 sujets (18%) avec des anomalies congénitales de C1 C2, chez 5 sujets (12%). 5 patients présentaient une instabilité uniquement en flexion et 3 patients présentaient une telle instabilité sur tous les clichés. 3 patients avec une instabilité occipito atloïdienne présentaient des anomalies de l’odontoide aggravant encore les conditions locales. Lorsqu’il existe une instabilité occipito atloïdienne, la distance C1 odontoide doit être évaluée car elle indique l’espace possible pour la moelle. Une spondylolyse cervicale a été relevée chez 16 patients (36% des sujets). Avec l’âge, les lésions dégénératives peuvent évoluer, survenant plus tôt que dans la population normale et peuvent léser les différents niveaux de la colonne cervicale. La moitié des patients avec une instabilité occipito atloïdienne ont une spondylolyse cervicale, avec une co-morbidité entraînant une moelle à risque.
Figures

Similar articles
-
Atlantoaxial instability in individuals with Down syndrome: epidemiologic, radiographic, and clinical studies.Pediatrics. 1987 Oct;80(4):555-60. Pediatrics. 1987. PMID: 2958770
-
Down syndrome. Cervical spine abnormalities and problems.Clin Pediatr (Phila). 1988 Sep;27(9):415-8. doi: 10.1177/000992288802700901. Clin Pediatr (Phila). 1988. PMID: 2970908
-
[Incidence of occipito-cervical instability in Down syndrome].Arch Neurobiol (Madr). 1990 Jan-Feb;53(1):33-7. Arch Neurobiol (Madr). 1990. PMID: 2144107 Spanish.
-
Cervical spine anomalies in children and adolescents.Curr Opin Pediatr. 2013 Feb;25(1):72-7. doi: 10.1097/MOP.0b013e32835bd4cf. Curr Opin Pediatr. 2013. PMID: 23263023 Review.
-
Evaluation of 2011 AAP cervical spine screening guidelines for children with Down Syndrome.Childs Nerv Syst. 2020 Nov;36(11):2609-2614. doi: 10.1007/s00381-020-04855-5. Epub 2020 Aug 10. Childs Nerv Syst. 2020. PMID: 32778937 Review.
Cited by
-
Prevalence of Common Disease Conditions in a Large Cohort of Individuals With Down Syndrome in the United States.J Patient Cent Res Rev. 2021 Apr 19;8(2):86-97. doi: 10.17294/2330-0698.1824. eCollection 2021 Spring. J Patient Cent Res Rev. 2021. PMID: 33898640 Free PMC article.
-
Anterior atlantoaxial subluxation with Down syndrome and arthritis: case report.J Spine Surg. 2018 Dec;4(4):803-809. doi: 10.21037/jss.2018.12.07. J Spine Surg. 2018. PMID: 30714014 Free PMC article.
-
Prevalence of upper cervical vertebral anomalies in children with non-syndromic cleft lip and/or palate in comparison with children without cleft in Iranian population.BMC Oral Health. 2025 Apr 19;25(1):602. doi: 10.1186/s12903-025-05798-6. BMC Oral Health. 2025. PMID: 40253336 Free PMC article.
-
Atlantoaxial subluxation and Down syndrome: A cross-sectional analysis.J Craniovertebr Junction Spine. 2024 Apr-Jun;15(2):173-177. doi: 10.4103/jcvjs.jcvjs_1_24. Epub 2024 May 24. J Craniovertebr Junction Spine. 2024. PMID: 38957770 Free PMC article.
-
Craniofacial and Airway Morphology in Down Syndrome: A Cone Beam Computed Tomography Case Series Evaluation.J Clin Med. 2024 Jul 3;13(13):3908. doi: 10.3390/jcm13133908. J Clin Med. 2024. PMID: 38999474 Free PMC article.
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/0270-3092(86)90019-6', 'is_inner': False, 'url': 'https://doi.org/10.1016/0270-3092(86)90019-6'}, {'type': 'PubMed', 'value': '2938541', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/2938541/'}]}
- Alvarez N, Rubin L (1986) Atlantoaxial instability in adults with Down syndrome: a clinical and radiological survey. Appl Res Ment Retard 7:67–78 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '7596705', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/7596705/'}]}
- American Academy of Pediatrics, Committee on Sports Medicine and Fitness (1995) Atlantoaxial instability in Down syndrome. Subject review. Pediatrics 96:151–154 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '2934395', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/2934395/'}]}
- Burke SW, French HG, Roberts JM, Johnston CE 2nd, Whitecloud TS 3rd, Edmunds JO Jr (1985) Chronic atlanto-axial instability in Down syndrome. J Bone Joint Surg Am 67:1356–1360 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PMC', 'value': 'PMC1029517', 'is_inner': False, 'url': 'https://pmc.ncbi.nlm.nih.gov/articles/PMC1029517/'}, {'type': 'PubMed', 'value': '8215544', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/8215544/'}]}
- Cremers MJ, Ramos L, Bol E, van Gijn J (1993) Radiological assessment of the atlantoaxial distance in Down’s syndrome. Arch Dis Child 69:347–350 - PMC - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '2136808', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/2136808/'}]}
- Crosby ET, Lui A (1990) The adult cervical spine: implications for airway management. Can J Anaesth 37:77–93 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
