

Consultations for middle ear disease, antibiotic prescribing and risk factors for reattendance: a case-linked cohort study
- PMID: 16536956
- PMCID: PMC1828259
Consultations for middle ear disease, antibiotic prescribing and risk factors for reattendance: a case-linked cohort study
Abstract
Background: Otitis media is the most common reason for children to receive antibiotics, but there is no evidence about the effect of prescribing on reattendance.
Aim: To evaluate the changing workload of middle ear disease in general practice, and the impact on surgery reattendance of prescribing antibiotics at first attendance.
Design of study: A case-linked cohort analysis for antibiotic prescribing versus no prescribing at first consultation event.
Setting: Two hundred and ninety-one practices spread throughout the UK recording for the General Practice Research Database (GPRD) and incorporating individual patient data records for 2,265,574 patients.
Method: All middle ear disease coded events that can be classed within acute otitis media (AOM) or glue ear sub-categories (and excluding chronic suppurative otitis media) were selected for analysis when the first event was from 1991-2001. The effect of antibiotic prescription on the risk of reattendance using Cox proportional hazards regression was analysed.
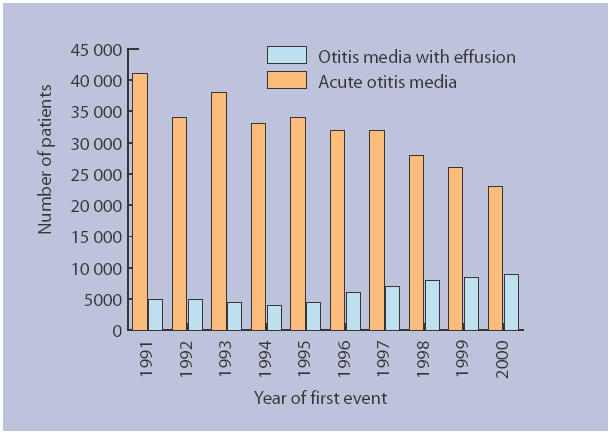
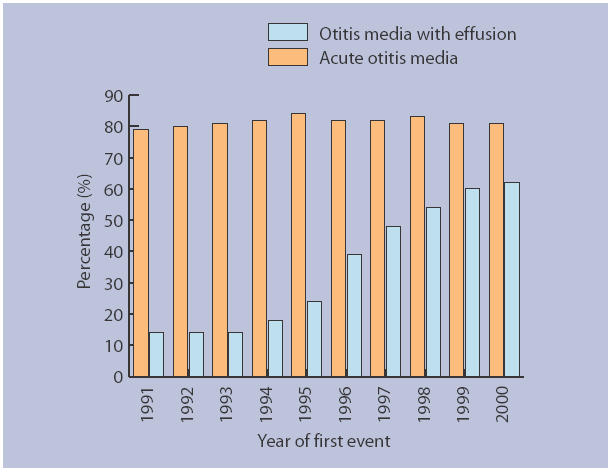
Results: Total consultations for AOM have fallen markedly over this decade, and glue ear consultations have risen but by a much smaller extent (26,000 decrease versus 4000 increase in consultations per year), which makes relabelling an unlikely explanation of the fall in AOM consultations. In the 2-10 years age range, consultations for AOM fell from 105.3 to 34.7 per 1000 per year, with glue ear consultations unaltered (15.2 to 16.7 per 1000 per year). Antibiotic prescribing for AOM has stayed remarkably constant (80-84% of consultations), but antibiotic prescribing for glue ear has risen sharply (13 to 62%). Prescribing antibiotics increased the risk of reattendance for AOM (hazard ratio [HR] = 1.09, 95% confidence interval [CI] = 1.07 to 1.10) and has reduced the risk of reattendance for glue ear (HR = 0.92, 95% CI = 0.88 to 0.96).
Conclusion: Prescribing antibiotics for AOM probably increased reattendance, but the opposite effect has been noted for glue ear, which suggests a treatment effect of antibiotics in glue ear. Further research is needed to clarify whether this possible benefit is worth the known harms, and if so in which subgroups of children.
Figures
Comment in
-
Prescribing antibiotics to patients with acute cough and otitis media.Br J Gen Pract. 2006 Mar;56(524):164-6. Br J Gen Pract. 2006. PMID: 16536953 Free PMC article. No abstract available.
-
Up-to-date findings show change in acute otitis media consultation trend.Br J Gen Pract. 2006 May;56(526):379-80. Br J Gen Pract. 2006. PMID: 16638257 Free PMC article. No abstract available.
References
-
- Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media. Pediatrics. 2004;113:1451–1465. - PubMed
-
- Stool SE, Berg AO, Berman S, et al. Otitis media with effusion in children. Guideline Technical Report, Number 12. Rockville MD: AHCPR; 1994. (95-0621)
-
- Haggard M, Hughes E. Objectives values and methods of screening childrens' hearing — a review of the literature. London: HMSO; 1991.
-
- Fergie N, Bayston R, Pearson JP, Birchall JP. Is otitis media with effusion a biofilm infection? Clin Otolaryngol. 2004;29:38–46. - PubMed
-
- Select Committee on Science and Technology. Resistance to antibiotics and other antimicrobial agents. 7th Report. London: HMSO; 1998. (HL 81-I)
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials