

Longer term outcomes from a randomised trial of prescribing strategies in otitis media
- PMID: 16536957
- PMCID: PMC1828260
Longer term outcomes from a randomised trial of prescribing strategies in otitis media
Abstract
Background: There are limited data about the longer-term outcomes in acute otitis media (AOM) when comparing the realistic alternatives of immediate prescription of antibiotics and a 'wait and see' or delayed prescribing policy.
Aim: The aim was to assess the medium and longer term outcomes of two prescribing strategies for otitis media.
Design of study: Follow-up of a randomised controlled trial cohort.
Setting: Primary care.
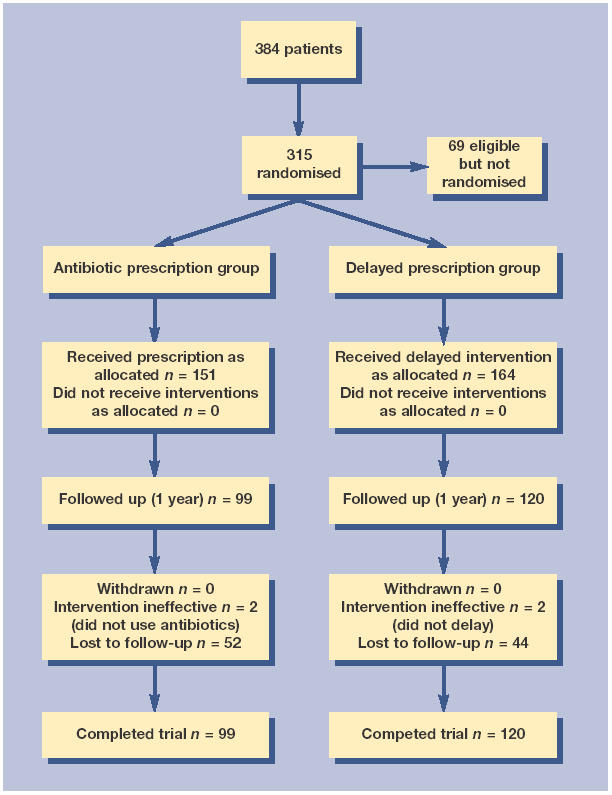
Method: Three-hundred and fifteen children aged 6 months to 10 years presenting with AOM were randomised to immediate antibiotics, or antibiotics delayed at the parents discretion 72 hours if the child still had significant otalgia or fever, or was not improving. Episodes of earache since study entry were documented, and a poor score (of 9 or more--the top 20%) on a reliable six-item functional rating scale (Cronbach's alpha = 0.75).
Results: The delayed prescribing strategy did not significantly increase reported episodes of earache in the 3 months since randomisation (odds ratio [OR] = 0.89; 95% confidence interval [CI] = 0.48 to 1.65) or over 1 year (OR = 1.03; 95% CI = 0.60 to 1.78) nor of poor scores on the function scale at 3 months (OR = 1.16; 95% CI = 0.61 to 2.22) or 1 year (OR = 1.12; 95% CI = 0.57 to 2.19), and controlling for subsequent antibiotic use after the randomised episode did not alter these estimates. The number of prior episodes of AOM documented in the doctor's notes predicted episodes of earache reported (0, 1, > or = 2 episodes, respectively; OR = 1, 2.42, 2.61; chi2 for trend 8.04; P<0.01). There was weaker evidence that prior episodes also predicted poor function at 1 year (OR = 1, 1.86, 2.28; chi2 for trend 5.49; P = 0.019). For children with recurrent AOM (two or more previous episodes documented in the doctor's notes, n = 43) there was possible evidence of fewer episodes of earache in the 3 months since study entry in the immediate antibiotic group (10% compared to 39% in the delayed group, chi2 4.8, P = 0.029), but no effect from randomisation to 1 year.
Conclusions: For most children, delayed prescribing is not likely to have adverse longer-term consequences. Children with recurrent AOM are more likely to have poorer outcomes. Secondary analysis should be treated with caution and requires confirmation, but suggests that treating such children with antibiotics immediately may not alter longer-term outcomes.
Figures
Comment in
-
Prescribing antibiotics to patients with acute cough and otitis media.Br J Gen Pract. 2006 Mar;56(524):164-6. Br J Gen Pract. 2006. PMID: 16536953 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials