

An acute graft-versus-host disease activity index to predict survival after hematopoietic cell transplantation with myeloablative conditioning regimens
- PMID: 16537799
- PMCID: PMC1895493
- DOI: 10.1182/blood-2006-01-0254
An acute graft-versus-host disease activity index to predict survival after hematopoietic cell transplantation with myeloablative conditioning regimens
Abstract
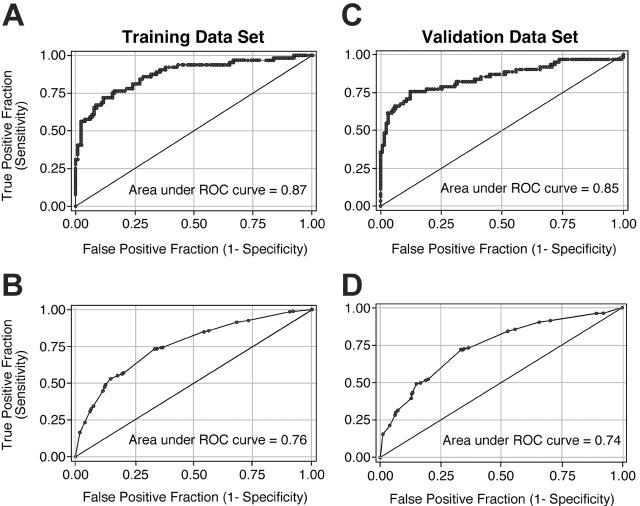
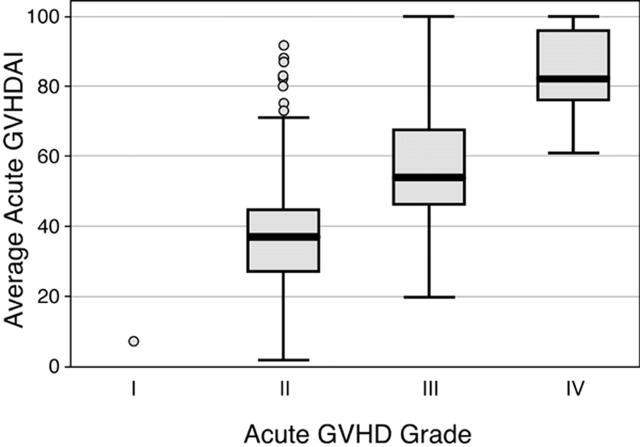
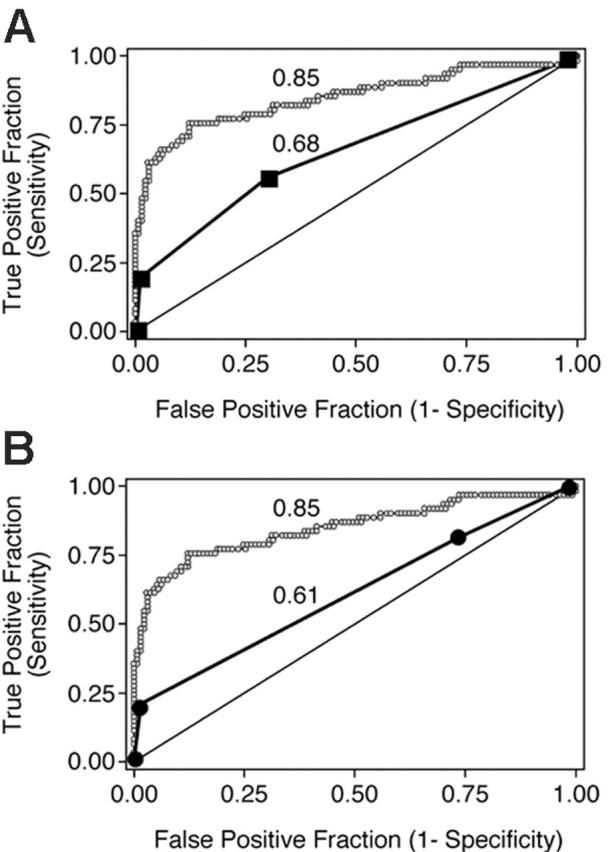
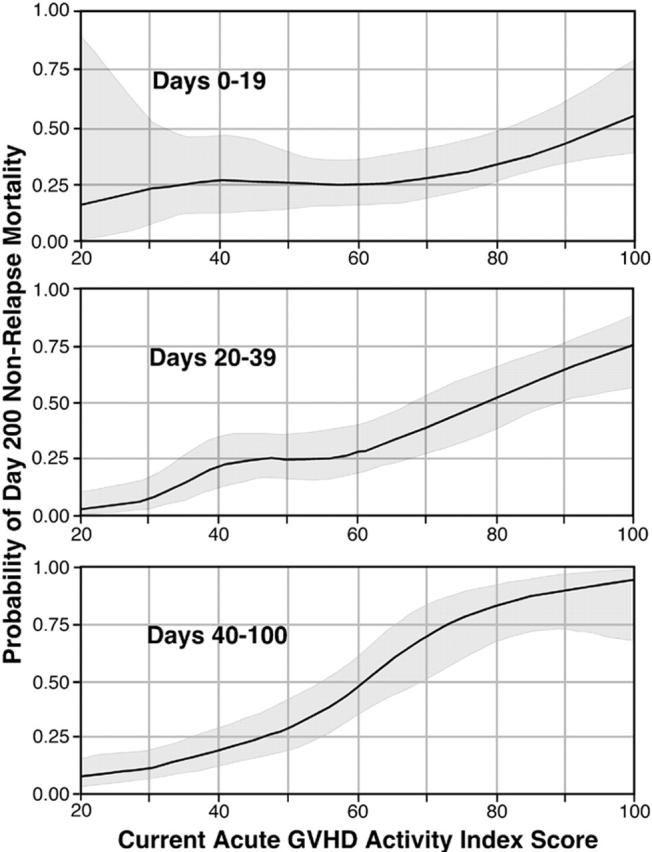
Algorithms for grading acute graft-versus-host disease (GVHD) are inaccurate in assessing mortality risk. We developed a method to predict mortality by using data from 386 patients with acute GVHD. From the onset of GVHD to day 100, GVHD manifestations were scored for the skin, liver, and upper and lower gastrointestinal tract, and data were recorded for immunosuppressive treatment, performance, and fever. Logistic regression models predicting nonrelapse mortality (NRM) at day 200 were developed with data from 193 randomly selected patients and then validated in the remaining 193 patients. Clinical parameters were grouped to optimize predictive accuracy measured as the area under a receiver-operator characteristic (ROC) curve. The optimal model included the total serum bilirubin concentration, oral intake, need for treatment with prednisone, and performance score. When the overall burden of GVHD was measured by using average Acute GVHD Activity Index (aGVHDAI) scores for each patient in training and validation data sets, areas under ROC curves were 0.87 and 0.85, respectively. Contour lines were generated to reflect the predicted NRM at day 200 as a function of current aGVHDAI scores. These results demonstrate that clinical manifestations of GVHD severity can be used to accurately predict the risk of NRM in real time.
Figures
References
-
- Martin PJ, McDonald GB, Sanders JE, et al. Increasingly frequent diagnosis of acute graft-versus-host disease after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2004;10: 320-327. - PubMed
-
- Sullivan KM. Graft versus host disease. In: Blume K, Forman SJ, Appelbaum F, eds. Thomas' Hematopoietic Cell Transplantation, ed 3. Malden, MA: Blackwell Publishing; 2004: 635-664.
-
- Glucksberg H, Storb R, Fefer A, et al. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation. 1974;18: 295-304. - PubMed
-
- Przepiorka D, Weisdorf D, Martin P, et al. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995;15: 825-828. - PubMed
-
- Rowlings PA, Przepiorka D, Klein JP, et al. IB-MTR Severity Index for grading acute graft-versus-host disease: retrospective comparison with Glucksberg grade. Br J Haematol. 1997;97: 855-864. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
