

A Markov computer simulation model of the economics of neuromuscular blockade in patients with acute respiratory distress syndrome
- PMID: 16539706
- PMCID: PMC1431518
- DOI: 10.1186/1472-6947-6-15
A Markov computer simulation model of the economics of neuromuscular blockade in patients with acute respiratory distress syndrome
Abstract
Background: Management of acute respiratory distress syndrome (ARDS) in the intensive care unit (ICU) is clinically challenging and costly. Neuromuscular blocking agents may facilitate mechanical ventilation and improve oxygenation, but may result in prolonged recovery of neuromuscular function and acute quadriplegic myopathy syndrome (AQMS). The goal of this study was to address a hypothetical question via computer modeling: Would a reduction in intubation time of 6 hours and/or a reduction in the incidence of AQMS from 25% to 21%, provide enough benefit to justify a drug with an additional expenditure of $267 (the difference in acquisition cost between a generic and brand name neuromuscular blocker)?
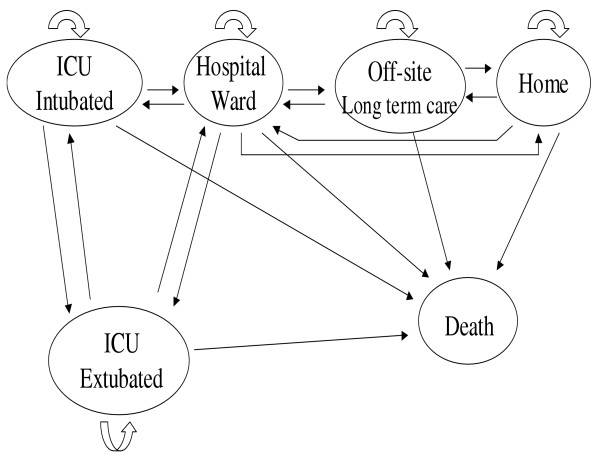
Methods: The base case was a 55 year-old man in the ICU with ARDS who receives neuromuscular blockade for 3.5 days. A Markov model was designed with hypothetical patients in 1 of 6 mutually exclusive health states: ICU-intubated, ICU-extubated, hospital ward, long-term care, home, or death, over a period of 6 months. The net monetary benefit was computed.
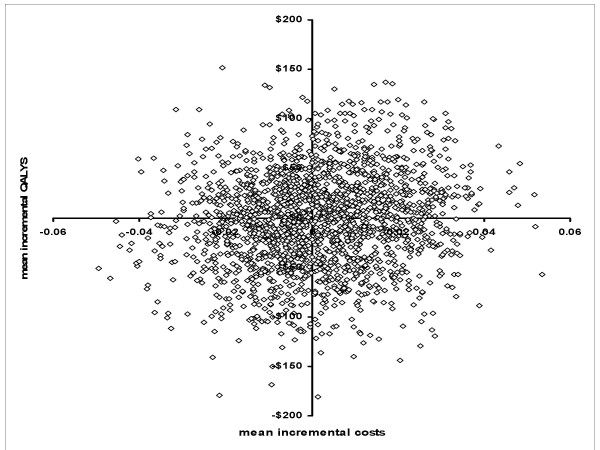
Results: Our computer simulation modeling predicted the mean cost for ARDS patients receiving standard care for 6 months to be $62,238 (5%-95% percentiles $42,259-$83,766), with an overall 6-month mortality of 39%. Assuming a ceiling ratio of $35,000, even if a drug (that cost $267 more) hypothetically reduced AQMS from 25% to 21% and decreased intubation time by 6 hours, the net monetary benefit would only equal $137.
Conclusion: ARDS patients receiving a neuromuscular blocker have a high mortality, and unpredictable outcome, which results in large variability in costs per case. If a patient dies, there is no benefit to any drug that reduces ventilation time or AQMS incidence. A prospective, randomized pharmacoeconomic study of neuromuscular blockers in the ICU to asses AQMS or intubation times is impractical because of the highly variable clinical course of patients with ARDS.
Figures
Similar articles
-
What Is the Evidence for Harm of Neuromuscular Blockade and Corticosteroid Use in the Intensive Care Unit?Semin Respir Crit Care Med. 2016 Feb;37(1):51-6. doi: 10.1055/s-0035-1570355. Epub 2016 Jan 28. Semin Respir Crit Care Med. 2016. PMID: 26820274 Review.
-
To Block or Not: Updates in Neuromuscular Blockade in Acute Respiratory Distress Syndrome.Ann Pharmacother. 2020 Sep;54(9):899-906. doi: 10.1177/1060028020910132. Epub 2020 Feb 28. Ann Pharmacother. 2020. PMID: 32111121 Review.
-
Acute lung injury and acute respiratory distress syndrome requiring tracheal intubation and mechanical ventilation in the intensive care unit: impact on managing uncertainty for patient-centered communication.Am J Hosp Palliat Care. 2013 Sep;30(6):569-75. doi: 10.1177/1049909112460566. Epub 2012 Sep 25. Am J Hosp Palliat Care. 2013. PMID: 23015728 Review.
-
Cost Analysis of Noninvasive Helmet Ventilation Compared with Use of Noninvasive Face Mask in ARDS.Can Respir J. 2018 Feb 8;2018:6518572. doi: 10.1155/2018/6518572. eCollection 2018. Can Respir J. 2018. PMID: 29670676 Free PMC article.
-
Acute Management and Long-Term Survival Among Subjects With Severe Middle East Respiratory Syndrome Coronavirus Pneumonia and ARDS.Respir Care. 2016 Mar;61(3):340-8. doi: 10.4187/respcare.04325. Epub 2015 Dec 23. Respir Care. 2016. PMID: 26701365
Cited by
-
Valuing COVID-19 Morbidity Risk Reductions.J Benefit Cost Anal. 2022 Summer;13(2):247-268. doi: 10.1017/bca.2022.11. Epub 2022 Aug 3. J Benefit Cost Anal. 2022. PMID: 36090595 Free PMC article.
-
Cost-effectiveness of the adjuvanted quadrivalent influenza vaccine for older adults in South Korea.Hum Vaccin Immunother. 2024 Dec 31;20(1):2348124. doi: 10.1080/21645515.2024.2348124. Epub 2024 May 7. Hum Vaccin Immunother. 2024. PMID: 38714332 Free PMC article.
-
Heterogenous treatment effect of neuromuscular blocking agents for moderate-to-severe ARDS: a post hoc Markov model re-analysis of the ACURASYS trial.Intensive Care Med. 2025 Sep;51(9):1615-1627. doi: 10.1007/s00134-025-08064-z. Epub 2025 Aug 6. Intensive Care Med. 2025. PMID: 40768068 Clinical Trial.
-
Cost effectiveness of cetuximab concurrent with radiotherapy for patients with locally advanced head and neck cancer in Taiwan: a decision-tree analysis.Clin Drug Investig. 2011 Oct 1;31(10):717-26. doi: 10.2165/11588980-000000000-00000. Clin Drug Investig. 2011. PMID: 21744880
-
Cost-utility analysis of antiviral use under pandemic influenza using a novel approach - linking pharmacology, epidemiology and heath economics.Epidemiol Infect. 2018 Mar;146(4):496-507. doi: 10.1017/S0950268818000158. Epub 2018 Feb 15. Epidemiol Infect. 2018. PMID: 29446343 Free PMC article.
References
-
- Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M, LeGall JR, Morris A, Spragg R. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994;149:818–24. - PubMed
-
- De Jonghe B, Sharshar T, Lefaucheur JP, Authier FJ, Durand-Zaleski I, Boussarsar M, Cerf C, Renaud E, Mesrati F, Carlet J, Raphael JC, Outin H, Bastuji-Garin S, Groupe de Reflexion et d'Etude des Neuromyopathies en Reanimation Paresis acquired in the intensive care unit: a prospective multicenter study. JAMA. 2002;288:2859–67. doi: 10.1001/jama.288.22.2859. - DOI - PubMed
-
- Murray MJ, Cowen J, DeBlock H, Erstad B, Gray AW, Jr, Tescher AN, McGee WT, Prielipp RC, Susla G, Jacobi J, Nasraway SA, Jr, Lumb PD, Task Force of the American College of Critical Care Medicine (ACCM) of the Society of Critical Care Medicine (SCCM), American Society of Health-System Pharmacists, American College of Chest Physicians Clinical practice guidelines for sustained neuromuscular blockade in the adult critically ill patient. Crit Care Med. 2002;30:142–56. doi: 10.1097/00003246-200201000-00021. - DOI - PubMed
-
- Prielipp RC, Coursin DB, Scuderi PE, Bowton DL, Ford SR, Cardenas VJ, Jr, Vender J, Howard D, Casale EJ, Murray MJ. Comparison of the infusion requirements and recovery profiles of vecuronium and cisatracurium 51W89 in intensive care unit patients. Anesth Analg. 1995;81:3–12. doi: 10.1097/00000539-199507000-00002. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
