

Esophageal and transpulmonary pressures in acute respiratory failure
- PMID: 16540960
- PMCID: PMC2278169
- DOI: 10.1097/01.CCM.0000215515.49001.A2
Esophageal and transpulmonary pressures in acute respiratory failure
Abstract
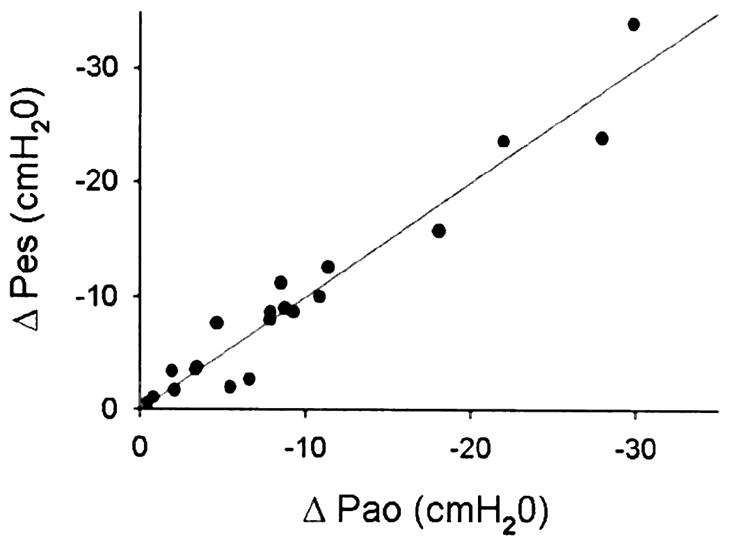
Objective: Pressure inflating the lung during mechanical ventilation is the difference between pressure applied at the airway opening (Pao) and pleural pressure (Ppl). Depending on the chest wall's contribution to respiratory mechanics, a given positive end-expiratory and/or end-inspiratory plateau pressure may be appropriate for one patient but inadequate or potentially injurious for another. Thus, failure to account for chest wall mechanics may affect results in clinical trials of mechanical ventilation strategies in acute respiratory distress syndrome. By measuring esophageal pressure (Pes), we sought to characterize influence of the chest wall on Ppl and transpulmonary pressure (PL) in patients with acute respiratory failure.
Design: Prospective observational study.
Setting: Medical and surgical intensive care units at Beth Israel Deaconess Medical Center.
Patients: Seventy patients with acute respiratory failure.
Interventions: Placement of esophageal balloon-catheters.
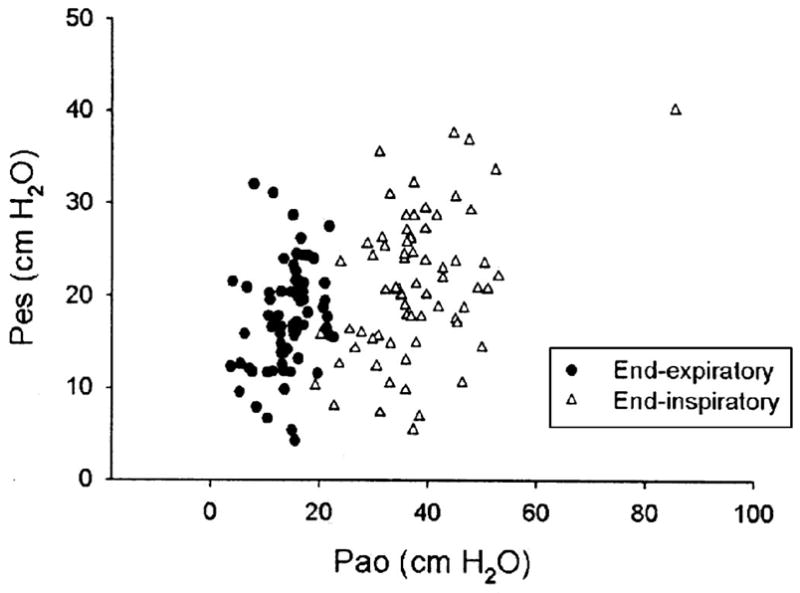
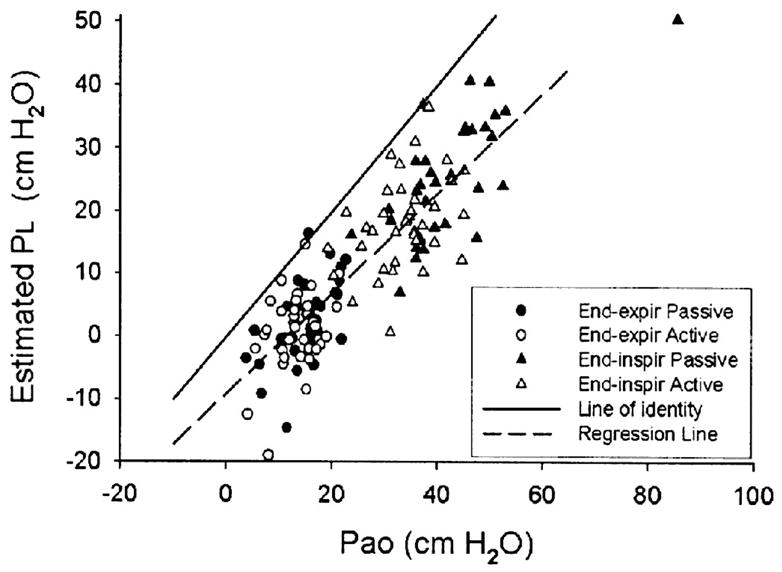
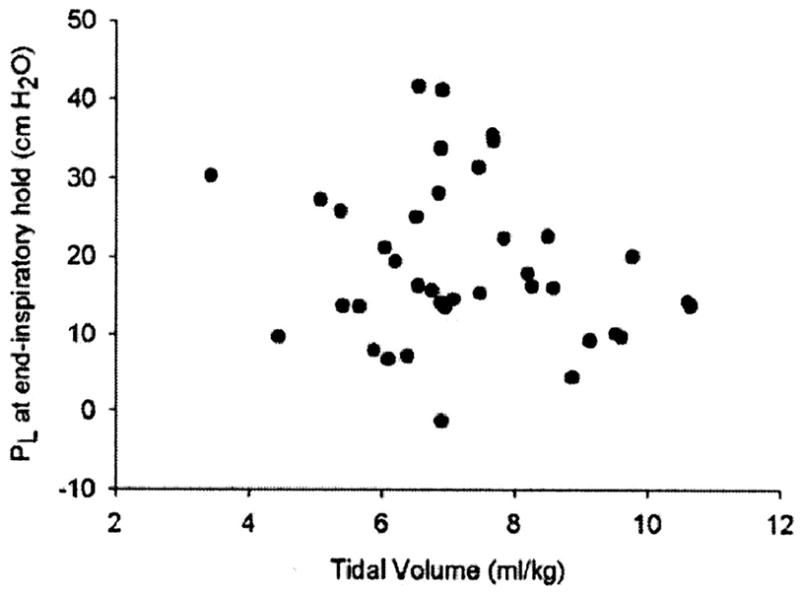
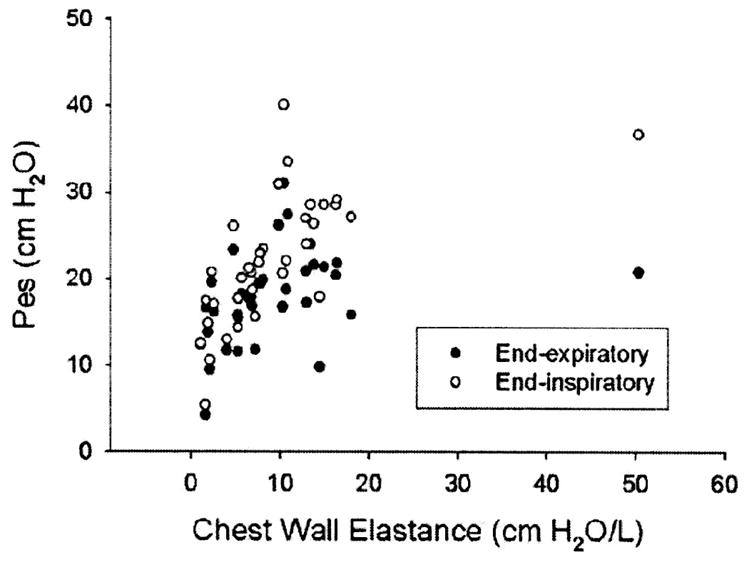
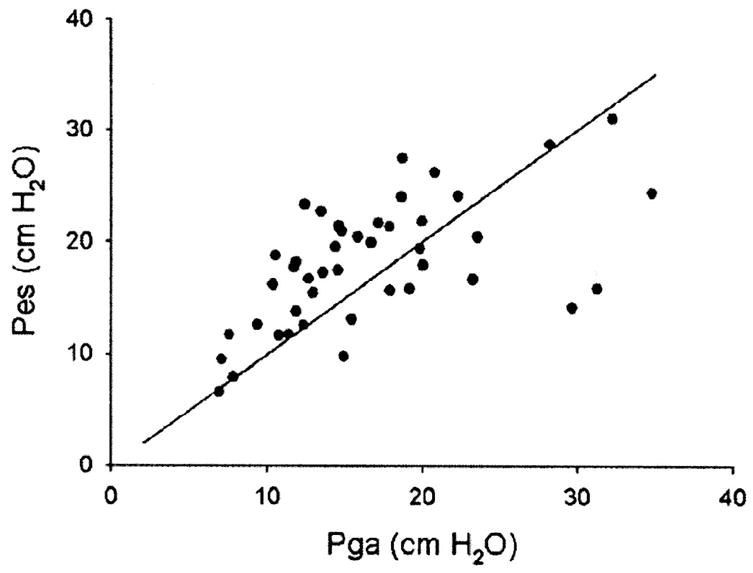
Measurements and main results: Airway, esophageal, and gastric pressures recorded at end-exhalation and end-inflation Pes averaged 17.5 +/- 5.7 cm H2O at end-expiration and 21.2 +/- 7.7 cm H2O at end-inflation and were not significantly correlated with body mass index or chest wall elastance. Estimated PL was 1.5 +/- 6.3 cm H2O at end-expiration, 21.4 +/- 9.3 cm H2O at end-inflation, and 18.4 +/- 10.2 cm H2O (n = 40) during an end-inspiratory hold (plateau). Although PL at end-expiration was significantly correlated with positive end-expiratory pressure (p < .0001), only 24% of the variance in PL was explained by Pao (R = .243), and 52% was due to variation in Pes.
Conclusions: In patients in acute respiratory failure, elevated esophageal pressures suggest that chest wall mechanical properties often contribute substantially and unpredictably to total respiratory impedance, and therefore Pao may not adequately predict PL or lung distention. Systematic use of esophageal manometry has the potential to improve ventilator management in acute respiratory failure by providing more direct assessment of lung distending pressure.
Figures
Comment in
-
Customizing lung-protective mechanical ventilation strategies.Crit Care Med. 2006 May;34(5):1554-5. doi: 10.1097/01.CCM.0000216183.25478.03. Crit Care Med. 2006. PMID: 16633256 No abstract available.
-
Esophageal and transpulmonary pressure help optimize mechanical ventilation in patients with acute lung injury.Crit Care Med. 2006 May;34(5):1556-8. doi: 10.1097/01.CCM.0000216146.51250.8D. Crit Care Med. 2006. PMID: 16633257 No abstract available.
References
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342:1334–1349. - PubMed
-
- Amato MB, Barbas CS, Medeiros DM, et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;338:347–354. - PubMed
-
- Chu EK, Whitehead T, Slutsky AS. Effects of cyclic opening and closing at low- and high-volume ventilation on bronchoalveolar lavage cytokines. Crit Care Med. 2004;32:168–174. - PubMed
-
- Slutsky AS. Lung injury caused by mechanical ventilation. Chest. 1999;116(1 Suppl):9S–15S. - PubMed
-
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
