

Antithrombin supplementation for anticoagulation during continuous hemofiltration in critically ill patients with septic shock: a case-control study
- PMID: 16542495
- PMCID: PMC1550897
- DOI: 10.1186/cc4853
Antithrombin supplementation for anticoagulation during continuous hemofiltration in critically ill patients with septic shock: a case-control study
Abstract
Introduction: Acquired antithrombin III (AT) deficiency may induce heparin resistance and premature membrane clotting during continuous renal replacement therapy (CRRT). The purpose of this study was to evaluate the effect of AT supplementation on filter lifespan in critically ill patients with septic shock requiring CRRT.
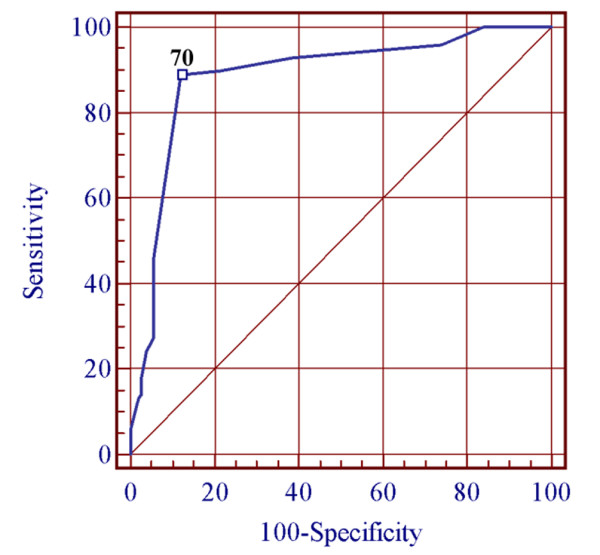
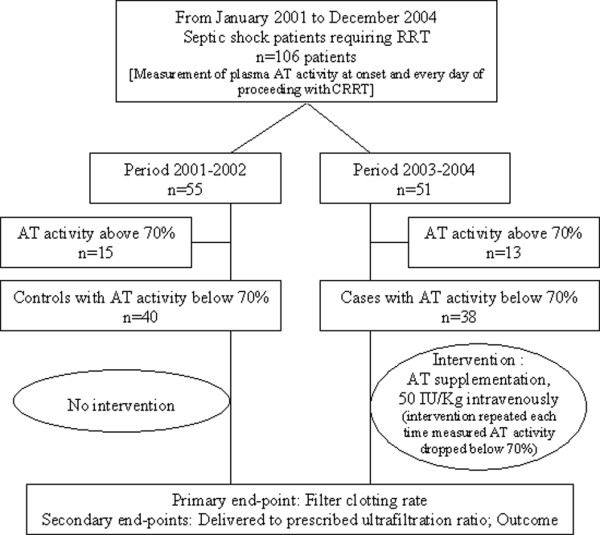
Methods: We conducted a retrospective case-control analysis based on a 4-year observational study with prospectively collected data in two medical intensive care units in a university hospital. In all, 106 patients with septic shock underwent CRRT during the study period (55 during 2001 to 2002 and 51 during 2003 to 2004). Of these, 78 had acquired AT deficiency (plasma level below 70%) at onset of renal supportive therapy, 40 in the first 2-year period and 38 in the last 2-year period. In the latter intervention period, patients received AT supplementation (50 IU/kg) during CRRT each time that plasma AT activity, measured once daily, fell below 70%.
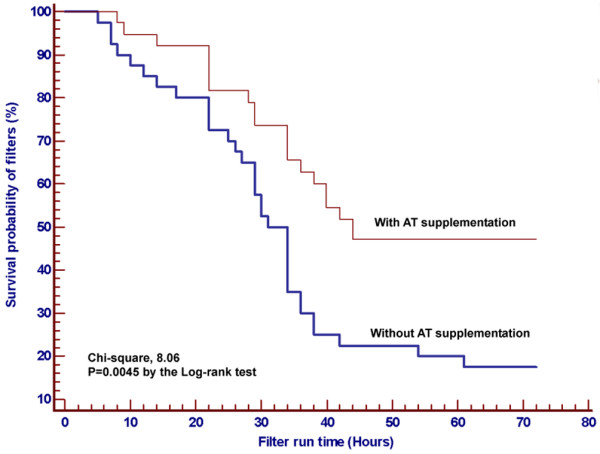
Results: In a case-control analysis of the 78 patients with acquired AT deficiency, groups were similar for baseline characteristics, except in severity of illness as assessed by a higher Simplified Acute Physiology Score (SAPS) II after 2002. In comparison with controls, cases had a significantly greater AT level after AT supplementation, but not at baseline, and a smaller number of episodes of clots, without excess bleeding risk. The median hemofilter survival time was longer in the AT group than in the heparin group (44.5 versus 33.4 hours; p = 0.0045). The hemofiltration dose, assessed by the ratio of delivered to prescribed ultrafiltration, increased during intervention. AT supplementation was independently associated with a decrease in clotting rate, whereas femoral angioaccess and higher SAPS II were independent predictors of filter failure. However, mortality did not differ between periods, in the control period the observed mortality was significantly higher than predicted by the SAPS II score, unlike in the treatment period.
Conclusion: In sepsis patients requiring CRRT and with acquired AT deficiency, anticoagulation with unfractionated heparin plus AT supplementation prevent premature filter clotting and may contribute to improving outcome, but the cost-effectiveness of AT remains to be determined.
Figures
Similar articles
-
Acquired deficit of antithrombin and role of supplementation in septic patients during continuous veno-venous hemofiltration.ASAIO J. 2008 Jan-Feb;54(1):124-8. doi: 10.1097/MAT.0b013e31815cc3bf. ASAIO J. 2008. PMID: 18204328
-
Continuous renal replacement therapies: anticoagulation in the critically ill at high risk of bleeding.J Nephrol. 2003 Jul-Aug;16(4):566-71. J Nephrol. 2003. PMID: 14696760
-
Predictive value of RIFLE classification on prognosis of critically ill patients with acute kidney injury treated with continuous renal replacement therapy.Chin Med J (Engl). 2009 May 5;122(9):1020-5. Chin Med J (Engl). 2009. PMID: 19493435
-
Heparin versus citrate for anticoagulation in critically ill patients treated with continuous renal replacement therapy.Nurs Crit Care. 2009 Jul-Aug;14(4):191-9. doi: 10.1111/j.1478-5153.2009.00339.x. Nurs Crit Care. 2009. PMID: 19531037 Review.
-
Continuous venovenous hemofiltration with citrate-based replacement fluid: efficacy, safety, and impact on nutrition.Am J Kidney Dis. 2005 Nov;46(5):908-18. doi: 10.1053/j.ajkd.2005.08.010. Am J Kidney Dis. 2005. PMID: 16253732 Review.
Cited by
-
Antithrombin Therapy: Current State and Future Outlook.Clin Appl Thromb Hemost. 2023 Jan-Dec;29:10760296231205279. doi: 10.1177/10760296231205279. Clin Appl Thromb Hemost. 2023. PMID: 37822179 Free PMC article.
-
Non anti-coagulant factors associated with filter life in continuous renal replacement therapy (CRRT): a systematic review and meta-analysis.BMC Nephrol. 2017 Feb 20;18(1):69. doi: 10.1186/s12882-017-0445-5. BMC Nephrol. 2017. PMID: 28219324 Free PMC article.
-
Four-day antithrombin therapy does not seem to attenuate hypercoagulability in patients suffering from sepsis.Crit Care. 2006;10(6):R160. doi: 10.1186/cc5098. Crit Care. 2006. PMID: 17107615 Free PMC article. Clinical Trial.
-
Antithrombin level and circuit thrombosis during hemofiltration after cardiopulmonary bypass.Intensive Care Med. 2008 Nov;34(11):2068-75. doi: 10.1007/s00134-008-1181-x. Epub 2008 Jun 25. Intensive Care Med. 2008. PMID: 18575842
-
Postoperative activity, but not preoperative activity, of antithrombin is associated with major adverse cardiac events after coronary artery bypass graft surgery.Anesth Analg. 2010 Oct;111(4):862-9. doi: 10.1213/ANE.0b013e3181b7908c. Epub 2009 Oct 9. Anesth Analg. 2010. PMID: 19820236 Free PMC article. Clinical Trial.
References
-
- Seitz R, Wolf M, Egbring R, Havemann K. The disturbance of hemostasis in septic shock: role of neutrophil elastase and thrombin, effects of antithrombin III and plasma substitution. Eur J Haematol. 1989;43:22–28. - PubMed
-
- Wilson RF, Mammen EF, Robson MC, Heggers JP, Soullier G, DePoli PA. Antithrombin, prekallikrein, and fibronectin levels in surgical patients. Arch Surg. 1986;121:635–640. - PubMed
-
- Fourrier F, Chopin C, Goudemand J, Hendrycx S, Caron C, Rime A, Marey A, Lestavel P. Septic shock, multiple organ failure, and disseminated intravascular coagulation. Compared patterns of antithrombin III, protein C, and protein S deficiencies. Chest. 1992;101:816–823. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
