

Circulating inflammatory mediators and organ dysfunction after cardiovascular surgery with cardiopulmonary bypass: a prospective observational study
- PMID: 16542504
- PMCID: PMC1550915
- DOI: 10.1186/cc4857
Circulating inflammatory mediators and organ dysfunction after cardiovascular surgery with cardiopulmonary bypass: a prospective observational study
Abstract
Introduction: Cardiovascular surgery with cardiopulmonary bypass (CPB) has improved in past decades, but inflammatory activation in this setting is still unpredictable and is associated with several postoperative complications. Perioperative levels of macrophage migration inhibitory factor (MIF) and other inflammatory mediators could be implicated in adverse outcomes in cardiac surgery.
Methods: Serum levels of MIF, monocyte chemoattractant protein (MCP)-1, soluble CD40 ligand, IL-6 and IL-10 from 93 patients subjected to CPB were measured by enzyme-linked immunosorbent assay and compared with specific and global postoperative organ dysfunctions through multiple organ dysfunction score (MODS) and sequential organ failure assessment (SOFA).
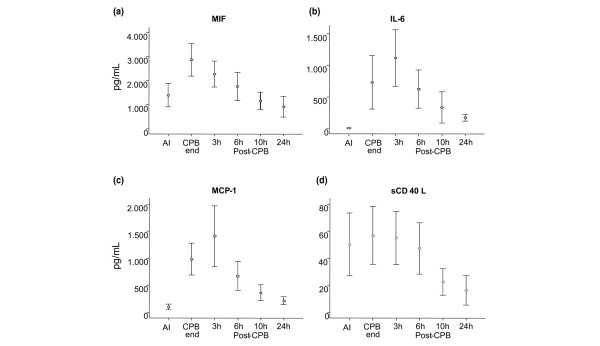
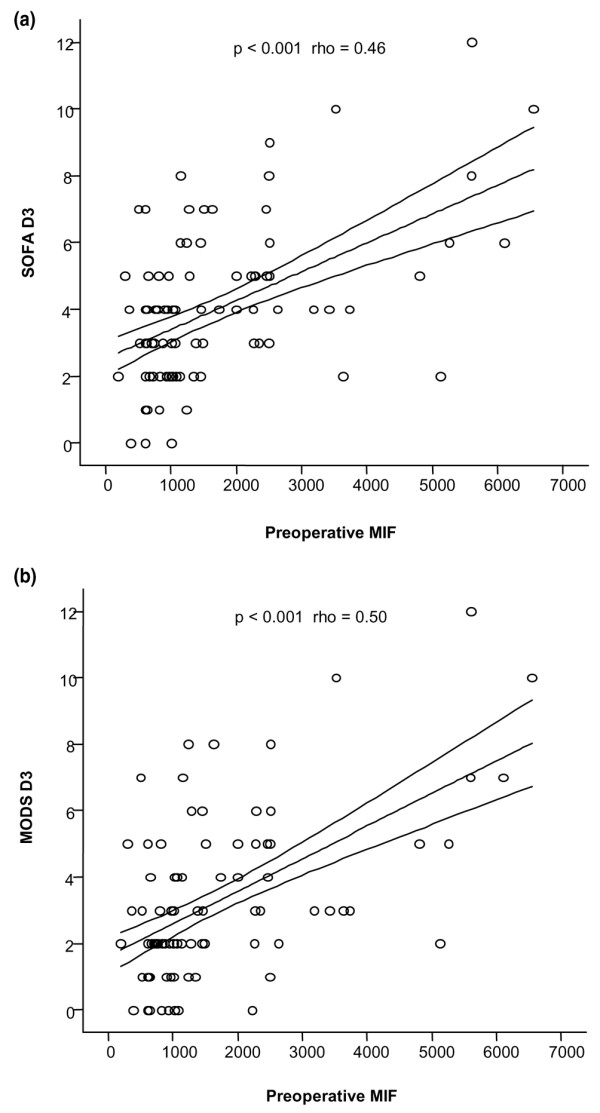
Results: Most of the cytokines measured had a peak of production between 3 and 6 hours after CPB, but maximum levels of MIF occurred earlier, at the cessation of CPB. Among specific organ dysfunctions, the most frequent was hematological, occurring in 82% of the patients. Circulatory impairment was observed in 73.1% of the patients, and 51% of these needed inotropics or vasopressors within the first 24 hours after surgery. The third most frequent dysfunction was pulmonary, occurring in 48.4% of the patients. Preoperative levels of MIF showed a relevant direct correlation with the intensity of global organ dysfunction measured by SOFA (rho = 0.46, p < 0.001) and MODS (rho = 0.50, p < 0.001) on the third day after surgery. MCP-1 production was associated with postoperative thrombocytopenia, and MIF was related to the use of a high dose of vasopressors in patients with cardiovascular impairment and also to lower values of the ratio of partial arterial oxygen tension (PaO2) to fraction of inspired oxygen (FiO2) registered in the first 24 hours after CPB.
Conclusion: Despite the multifactorial nature of specific or multiple organ dysfunctions, MIF should be explored as a predicting factor of organ dysfunction, or even as a potential therapeutic target in decreasing postoperative complications.
Figures
Comment in
-
Macrophage migration inhibitory factor: controller of systemic inflammation.Crit Care. 2006;10(2):138. doi: 10.1186/cc4899. Crit Care. 2006. PMID: 16677407 Free PMC article. Review.
Similar articles
-
Circulating cytokines, chemokines, and stress hormones are increased in patients with organ dysfunction following liver resection.J Surg Res. 2006 Jun 15;133(2):102-12. doi: 10.1016/j.jss.2005.10.025. Epub 2006 Jan 4. J Surg Res. 2006. PMID: 16386757
-
A single nucleotide polymorphism of macrophage migration inhibitory factor is related to inflammatory response in coronary bypass surgery using cardiopulmonary bypass.Eur J Cardiothorac Surg. 2006 Jul;30(1):59-63. doi: 10.1016/j.ejcts.2006.01.058. Epub 2006 Mar 9. Eur J Cardiothorac Surg. 2006. PMID: 16527487
-
Ventilation according to the open lung concept attenuates pulmonary inflammatory response in cardiac surgery.Eur J Cardiothorac Surg. 2005 Dec;28(6):889-95. doi: 10.1016/j.ejcts.2005.10.007. Epub 2005 Nov 3. Eur J Cardiothorac Surg. 2005. PMID: 16271479 Clinical Trial.
-
[The significance of neutrophil in inflammatory response after cardiac surgery with cardiopulmonary bypass].Wiad Lek. 2007;60(3-4):171-7. Wiad Lek. 2007. PMID: 17726872 Review. Polish.
-
Side effects of cardiopulmonary bypass: what is the reality?J Card Surg. 2004 Nov-Dec;19(6):481-8. doi: 10.1111/j.0886-0440.2004.04101.x. J Card Surg. 2004. PMID: 15548178 Review.
Cited by
-
Inflammation and Oxidative Stress in the Context of Extracorporeal Cardiac and Pulmonary Support.Front Immunol. 2022 Mar 4;13:831930. doi: 10.3389/fimmu.2022.831930. eCollection 2022. Front Immunol. 2022. PMID: 35309362 Free PMC article. Review.
-
Dynamic pituitary-adrenal interactions in response to cardiac surgery.Crit Care Med. 2015 Apr;43(4):791-800. doi: 10.1097/CCM.0000000000000773. Crit Care Med. 2015. PMID: 25517478 Free PMC article.
-
The role of CD74 in cardiovascular disease.Front Cardiovasc Med. 2023 Jan 12;9:1049143. doi: 10.3389/fcvm.2022.1049143. eCollection 2022. Front Cardiovasc Med. 2023. PMID: 36712241 Free PMC article. Review.
-
cfDNA correlates with endothelial damage after cardiac surgery with prolonged cardiopulmonary bypass and amplifies NETosis in an intracellular TLR9-independent manner.Sci Rep. 2017 Dec 12;7(1):17421. doi: 10.1038/s41598-017-17561-1. Sci Rep. 2017. PMID: 29234042 Free PMC article.
-
Wingless-related integration site (WNT) signaling is activated during the inflammatory response upon cardiac surgery: A translational study.Front Cardiovasc Med. 2022 Nov 11;9:997350. doi: 10.3389/fcvm.2022.997350. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36440011 Free PMC article.
References
-
- Butler J, Rocker GM, Westaby S. Inflammatory response to cardiopulmonary bypass. Ann Thorac Surg. 1993;55:552–559. - PubMed
-
- Andersen LW, Baek L, Degn H, Lehd J, Krasnik M, Rasmussen JP. Presence of circulating endotoxin during cardiac operations. J Thorac Cardiovasc Surg. 1987;93:115–119. - PubMed
-
- Gessler P, Pretre R, Hohl V, Rousson V, Fischer J, Dahinden C. CXC-chemokine stimulation of neutrophils correlates with plasma levels of myeloperoxidase and lactoferrin and contributes to clinical outcome after pediatric cardiac surgery. Shock. 2004;22:513–520. doi: 10.1097/01.shk.0000145939.54838.51. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
