

Newly expressed SUR1-regulated NC(Ca-ATP) channel mediates cerebral edema after ischemic stroke
- PMID: 16550187
- PMCID: PMC2740734
- DOI: 10.1038/nm1390
Newly expressed SUR1-regulated NC(Ca-ATP) channel mediates cerebral edema after ischemic stroke
Abstract
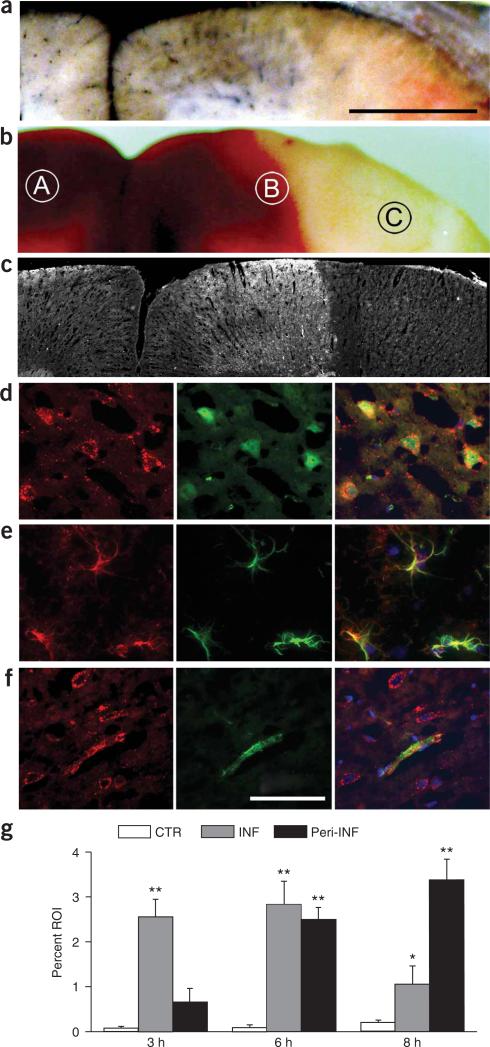
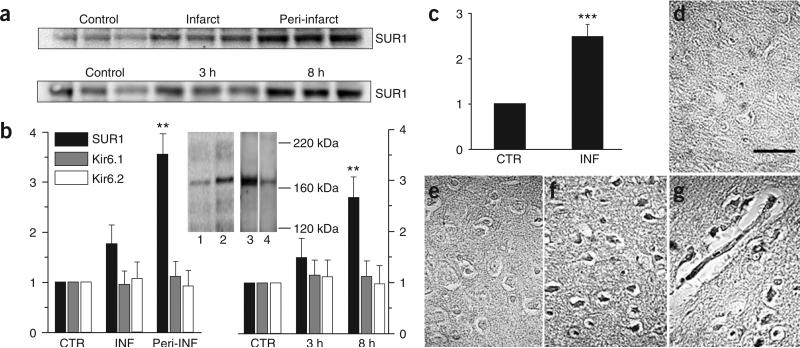
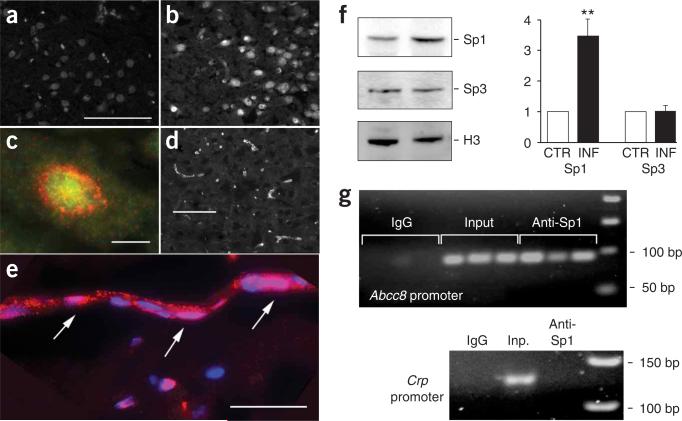
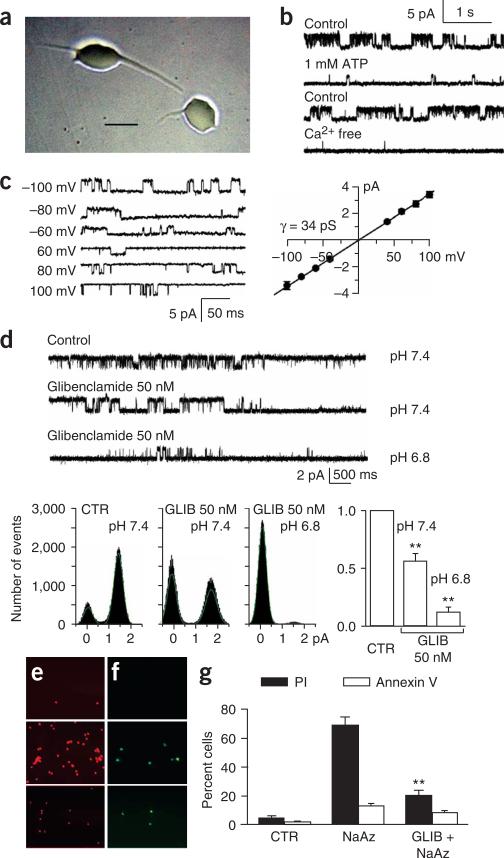
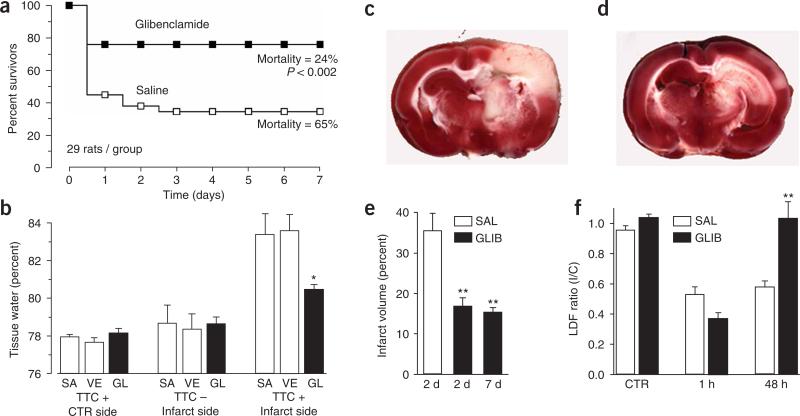
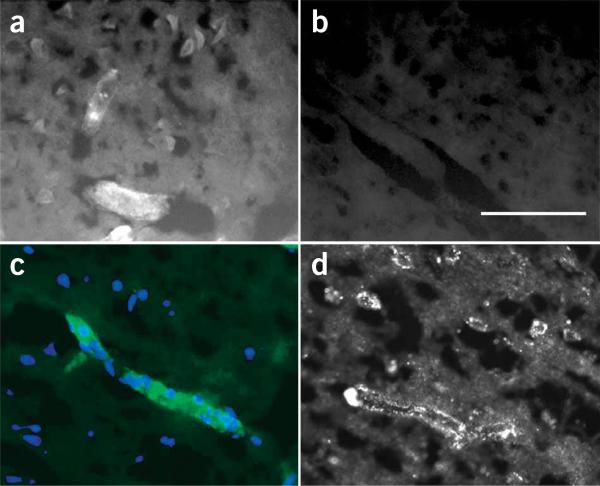
Pathological conditions in the central nervous system, including stroke and trauma, are often exacerbated by cerebral edema. We recently identified a nonselective cation channel, the NC(Ca-ATP) channel, in ischemic astrocytes that is regulated by sulfonylurea receptor 1 (SUR1), is opened by depletion of ATP and, when opened, causes cytotoxic edema. Here, we evaluated involvement of this channel in rodent models of stroke. SUR1 protein and mRNA were newly expressed in ischemic neurons, astrocytes and capillaries. Upregulation of SUR1 was linked to activation of the transcription factor Sp1 and was associated with expression of functional NC(Ca-ATP) but not K(ATP) channels. Block of SUR1 with low-dose glibenclamide reduced cerebral edema, infarct volume and mortality by 50%, with the reduction in infarct volume being associated with cortical sparing. Our findings indicate that the NC(Ca-ATP) channel is crucially involved in development of cerebral edema, and that targeting SUR1 may provide a new therapeutic approach to stroke.
Figures
References
-
- Ayata C, Ropper AH. Ischaemic brain oedema. J. Clin. Neurosci. 2002;9:113–124. - PubMed
-
- Seino S. ATP-sensitive potassium channels: a model of heteromultimeric potassium channel/receptor assemblies. Annu. Rev. Physiol. 1999;61:337–362. - PubMed
-
- Mathews KS, et al. Rapid quantification of ischaemic injury and cerebroprotection in brain slices using densitometric assessment of 2,3,5-triphenyltetrazolium chloride staining. J. Neurosci. Methods. 2000;102:43–51. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
