

Pneumonia severity index in the immunocompromised
- PMID: 16550266
- PMCID: PMC2539011
- DOI: 10.1155/2006/195464
Pneumonia severity index in the immunocompromised
Abstract
Background: The pneumonia severity index (PSI) accounts for many comorbidities, but not immunosuppression.
Objectives: To document the utility of the PSI to predict mortality in immunocompromised patients (IP) with community-acquired pneumonia (CAP).
Methods: Charts of 284 patients with immunosuppression and CAP were reviewed, and these patients were compared with a contemporary sample of non-IP with CAP. The ability of the PSI to predict mortality was assessed by using multiple logistic regression. Discrimination of the PSI was studied by using the concordance index.
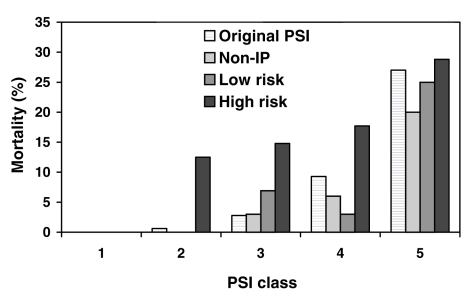
Results: Thirty-nine of 284 IP died. Mortality varied according to the etiology of the immunosuppression. Patients with HIV, solid organ transplantation or treatment with immunosuppressive drugs (n=118) had a low in-hospital mortality (4.3%) and were classified as low risk. IP with hematological malignancies, chemotherapy, chest radiation or marrow transplantation (n=166) had a high mortality (20%) and were classified as high risk. Compared with non-IP, low-risk IP had similar PSI-controlled mortality (OR=0.9, P=0.80), whereas high-risk IP had significantly greater mortality (OR=2.8, P<0.0001). The concordance index revealed similar discrimination for the PSI in low-risk IP (0.77) and in non-IP (0.7), but inferior discrimination in high-risk patients (0.6).
Conclusions: Patients with CAP and immunosuppression can be divided into low-risk and high-risk groups. The low-risk IP have mortality similar to non-IP and can be risk stratified by using the PSI.
HISTORIQUE: L’indice de gravité de la pneumonie (IGP) peut expliquer de nombreuses comorbidités, mais non l’immunosuppression.
OBJECTIFS: Documenter l’utilité de l’IGP à prédire la mortalité chez des sujets immunodéprimés atteints d’une pneumonie extrahospitalière (PEH).
MÉTHODES: Les dossiers de 284 patients immunodéprimés atteints d’une PEH ont été passés en revue et ces patients ont été comparés à un échantillon contemporain de sujets atteints de PEH non immunodéprimés. La valeur prédictive de l’IGP en regard de la mortalité a été évaluée par analyse de régression logistique multiple. Le seuil de mobilité de l’IGP a été étudié à l’aide de l’indice de concordance.
RÉSULTATS: Trente-neuf des patients immunodéprimés sur 284 sont décédés. La mortalité variait selon l’étiologie de l’immunosuppression. La présence du VIH, la greffe d’un organe plein ou le traitement immunosuppresseur (n = 118) ont donné lieu à un faible taux de mortalité durant l’hospitalisation (4,3 %) et on leur a assigné une catégorie de risque faible. L’immunosuppression associée aux cancers du sang, à la chimiothérapie, à la radiothérapie thoracique ou à la transplantation de moelle osseuse (n = 166) ont pour leur part donné lieu à un taux de mortalité élevé (20 %) et on leur a assigné une catégorie de risque élevé. Comparativement aux sujets non immunodéprimés, les sujets exposés à un risque faible présentaient le même taux de mortalité selon l’IGP (RR = 0,9, p = 0,80), alors que les sujets à haut risque présentaient un taux de mortalité beaucoup plus élevé (RR = 2,8, p < 0,0001). L’indice de concordance a révélé un seuil de mobilité similaire pour l’IGP chez les sujets immunodéprimés à risque faible (0,77) et chez les sujets non immunodéprimés (0,7), mais un seuil de mobilité plus faible pour les sujets à risque élevé (0,6).
CONCLUSIONS: Les patients immunodéprimés qui souffrent d’une PEH peuvent être subdivisés en deux groupes selon qu’ils sont exposés à un risque faible ou élevé. Les immunodéprimés à risque faible présentent le même taux de mortalité que les sujets non immunodéprimés et peuvent être stratifiés selon leur risque au moyen de l’IGP.
Figures
References
-
- Marston BJ, Plouffe JF, File TM, Jr, et al. The Community-Based Pneumonia Incidence Study Group. Incidence of community-acquired pneumonia requiring hospitalization. Results of a population-based active surveillance Study in Ohio. Arch Intern Med. 1997;157:1709–18. - PubMed
-
- Niederman MS, McCombs JS, Unger AN, Kumar A, Popovian R. The cost of treating community-acquired pneumonia. Clin Ther. 1998;20:820–37. - PubMed
-
- Lave JR, Lin CC, Fine MJ. The cost of treating patients with community-acquired pneumonia. Semin Respir Crit Care Med. 1999;20:189–98.
-
- Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997;336:243–50. - PubMed
-
- Ewig S, Ruiz M, Mensa J, et al. Severe community-acquired pneumonia. Assessment of severity criteria. Am J Respir Crit Care Med. 1998;158:1102–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
