

Case Reports
Isolated posterior cerebral artery dissection: report of three cases
Affiliations
- PMID: 16552010
- PMCID: PMC7976983
Item in Clipboard
Case Reports
Isolated posterior cerebral artery dissection: report of three cases
AJNR Am J Neuroradiol.
2006 Mar.
Abstract
Isolated dissection of the posterior cerebral artery (PCA) is a rare but important cause of stroke in younger patients, particularly women. We present 3 cases of dissection of the P2 segment of the PCA. In 2 patients, an association with minor axial head trauma was documented, suggesting shearing injury of the PCA as it crosses over the free edge of the tentorium. The clinical and imaging findings are discussed, and the therapeutic management is reviewed.
Figures
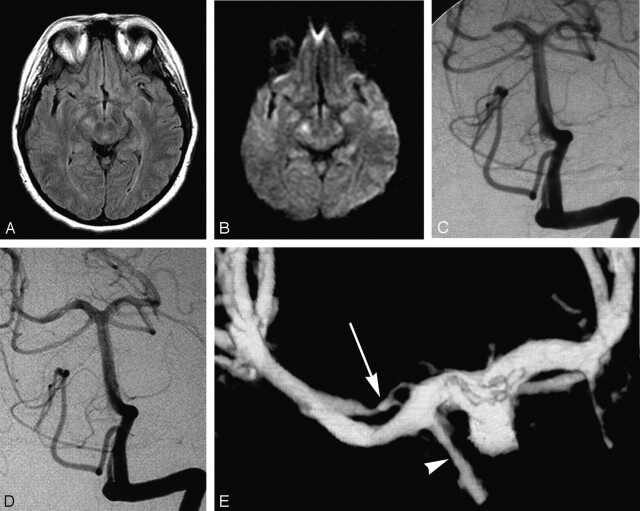
47-year-old woman presenting with quadranopsia. A, Axial FLAIR image demonstrating hyperintensity in the right cerebral peduncle. B, Axial diffusion-weighted image (DWI) image showing corresponding abnormal increased signal intensity. There was respective low signal intensity on the apparent diffusion coefficient map (not shown). C, DSA, left vertebral artery injection, transfacial view, demonstrates a smoothly tapered focal, near-occlusive narrowing of the proximal right PCA. D, DSA, left vertebral artery injection, transfacial view. One-year follow-up demonstrating a “double lumen” sign of the right P2 segment. E, 3D reconstruction of left vertebral angiogram rotational DSA which shows 2 patent lumens (double lumen sign) distal to the posterior communicating artery (arrowhead). Note the irregularly recanalized false lumen (arrow) with 2 separate inflow channels.
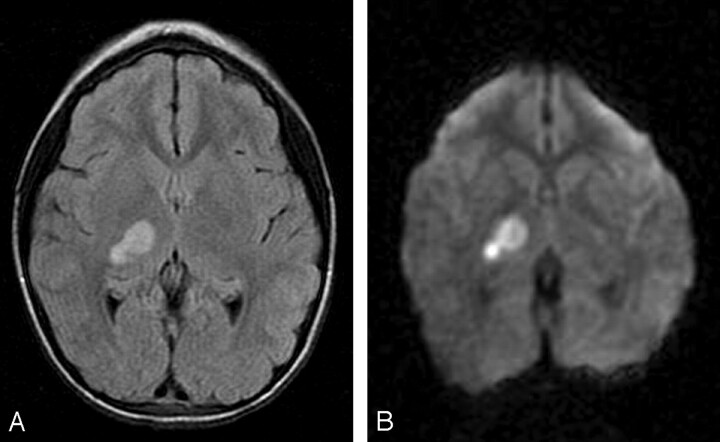
7-year-old girl presenting with left hemiparesis. A, Axial FLAIR image demonstrating hyperintensity in the right thalamus and posterior limb of the internal capsule. B, Axial DWI image showing corresponding restricted diffusion. There was respective low signal intensity on the apparent diffusion coefficient map (not shown). C, DSA, left vertebral artery injection, transfacial image demonstrating a focal narrowing and irregularity of the proximal right PCA.
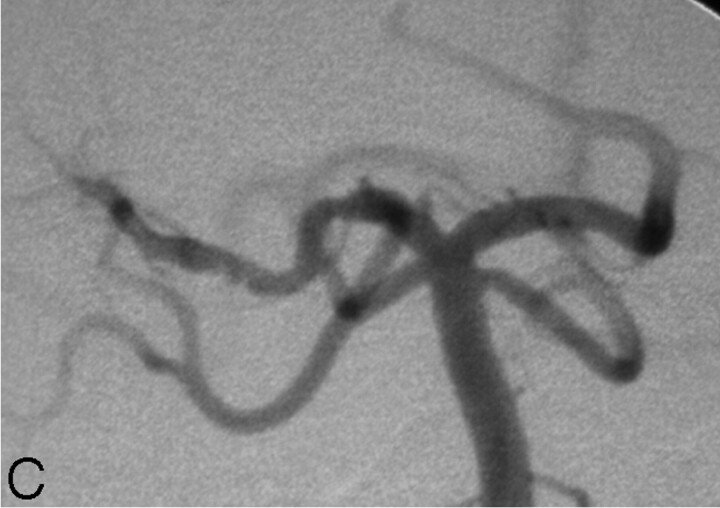
7-year-old girl presenting with left hemiparesis. A, Axial FLAIR image demonstrating hyperintensity in the right thalamus and posterior limb of the internal capsule. B, Axial DWI image showing corresponding restricted diffusion. There was respective low signal intensity on the apparent diffusion coefficient map (not shown). C, DSA, left vertebral artery injection, transfacial image demonstrating a focal narrowing and irregularity of the proximal right PCA.
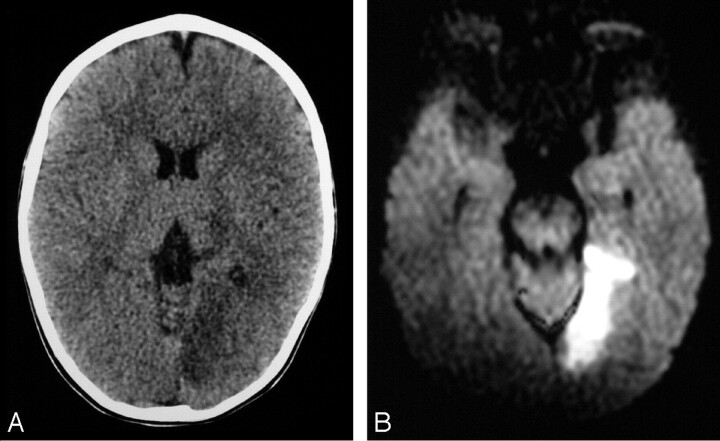
19-month old boy presenting with right hemiparesis. A, Axial noncontrast head CT demonstrating hypoattenuation in the medial aspect of the left occipital lobe involving the cortex and subcortical white matter with loss of gray-white matter differentiation. B, Axial DWI showing corresponding restricted diffusion compatible with infarct. There was respective low signal intensity on the apparent diffusion coefficient map (not shown). C, DSA, right vertebral artery injection, transfacial image demonstrating an irregular and narrowed left proximal PCA.

19-month old boy presenting with right hemiparesis. A, Axial noncontrast head CT demonstrating hypoattenuation in the medial aspect of the left occipital lobe involving the cortex and subcortical white matter with loss of gray-white matter differentiation. B, Axial DWI showing corresponding restricted diffusion compatible with infarct. There was respective low signal intensity on the apparent diffusion coefficient map (not shown). C, DSA, right vertebral artery injection, transfacial image demonstrating an irregular and narrowed left proximal PCA.
Similar articles
-
[Ischemic stroke due to isolated spontaneous posterior cerebral artery dissection in young adults].Zh Nevrol Psikhiatr Im S S Korsakova. 2009;109(5 Suppl 2):3-10. Zh Nevrol Psikhiatr Im S S Korsakova. 2009. PMID: 19894294 Russian.
-
[Isolated posterior cerebral artery dissection--case report and review of the literature].No Shinkei Geka. 2003 Jun;31(6):671-5. No Shinkei Geka. 2003. PMID: 12833877 Review. Japanese.
-
Dissection of bilateral intracranial vertebral artery with basilar artery involvement: a case report of a patient free from neurological deficits.Intern Med. 2007;46(17):1467-70. doi: 10.2169/internalmedicine.46.0210. Epub 2007 Sep 3. Intern Med. 2007. PMID: 17827851
-
Spontaneous basilar artery dissection.Hong Kong Med J. 2007 Apr;13(2):144-6. Hong Kong Med J. 2007. PMID: 17406043
-
[Isolated dissection of the posterior cerebral artery].Rev Neurol (Paris). 1996 Aug-Sep;152(8-9):542-7. Rev Neurol (Paris). 1996. PMID: 8991176 Review. French.
Cited by
-
Endovascular management for p2 aneurysms of the posterior cerebral artery. Experience on proximal occlusion of the p2 segmen.Interv Neuroradiol. 2009 Sep;15(3):341-8. doi: 10.1177/159101990901500313. Epub 2009 Nov 4. Interv Neuroradiol. 2009. PMID: 20465919 Free PMC article.
-
Subarachnoid hemorrhage from a dissecting aneurysm of the posterior cerebral artery in a child : rebleeding after stent-assisted coiling followed by stent-within-stent technique.J Korean Neurosurg Soc. 2011 Feb;49(2):134-8. doi: 10.3340/jkns.2011.49.2.134. Epub 2011 Feb 28. J Korean Neurosurg Soc. 2011. PMID: 21519506 Free PMC article.
-
State-of-art in surgical treatment of dissecting posterior circulation intracranial aneurysms.Neurosurg Rev. 2018 Jan;41(1):31-45. doi: 10.1007/s10143-016-0749-0. Epub 2016 May 24. Neurosurg Rev. 2018. PMID: 27215913 Review.
-
Optional Endovascular Therapy of Dissecting Posterior Cerebral Artery Aneurysm.Interv Neurol. 2017 Oct;6(3-4):219-228. doi: 10.1159/000477360. Epub 2017 Jun 17. Interv Neurol. 2017. PMID: 29118799 Free PMC article.
-
Isolated ipsilateral abducens nerve palsy and contralateral homonymous hemianopsia associated with unruptured posterior cerebral artery aneurysm: A rare neurological finding.J Cerebrovasc Endovasc Neurosurg. 2024 Sep;26(3):318-323. doi: 10.7461/jcen.2024.E2023.07.002. Epub 2024 Jan 22. J Cerebrovasc Endovasc Neurosurg. 2024. PMID: 38247033 Free PMC article.
References
-
- Scott GE, Neubuerger KT, Kenst J. Dissecting aneurysms of intracranial arteries. Neurology 1960;10:22–27 - PubMed
-
- Yonas H, Agamanolis D, Takaoka Y, et al. Dissecting aneurysms of the intracranial arteries. Surg Neurol 1977;8:407–15 - PubMed
-
- Johnson AC, Graves VB, Pfaff JP Jr. Dissecting aneurysms of intracranial arteries. Surg Neurol 1977;7:49–52 - PubMed
-
- Fisher CM, Ojemann RG, Roberson AG. Spontaneous dissection of the cervico-cerebral arteries. Can J Neurol Sci 1978;5:9–19 - PubMed
-
- Kulla L, Deymeer F, Smith TW, et al. Intracranial dissecting and saccular aneurysms in polycystic kidney disease: report of a case. Arch Neurol 1982;39:776–78 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical